MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
ASSISTANT EDITORS
EDITOR IN CHIEF
Blaga Vasile (electronic version)
Koren Rumelia
Andó Ottó (print version)
ASSISTANT EDITOR IN CHIEF
Oană Cristian Sever (editorialist)
Bumbulu Călin
Stăncioiu Tudor (Dental Medicine)
EDITORIAL BOARD
Bauer Adalbert (SCM Satu Mare, România)
Lup Liliana (Synevo Satu Mare, România)
Bidilean Nicolae (Emergency County Hospital,
Kesler Gavriel (Israel)
Satu Mare, România)
Kiss Ladislau (Emergency County Hospital,
Boros Melinda (Bucureşti, România)
Satu Mare, România)
Borcean Gheorghe (Caransebeş Hospital, România)
Mihalca Man Sorina (Emergency County Hospital,
Brândeu Ioan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Neumann Gad (Hasharon Hospital, Tel Aviv, Israel)
Cârstea Constantin (CMI Braşov, România)
Negru Alina (SCM Satu Mare, România)
Cojocaru Manole (Titu Maiorescu University,
Rath-Wolfson Lea (Hasharon Hospital, Tel Aviv, Israel)
Bucureşti, România)
Rădulescu Viorel (CMI Olt, România)
Comăneanu Raluca Monica (Titu Maiorescu University,
Roatiş Marius Dinu (Emergency County Hospital,
Bucureşti, România)
Satu Mare, România)
Cornean-Santa Corina (Emergency County Hospital,
Rusu Cristian Bogdan (Emergency County Hospital,
Satu Mare, România)
Satu Mare, România)
Feciche Bogdan (Emergency County Hospital,
Shvero Kesler Dana (Hadassa University, Jerusalem, Israel)
Satu Mare, România)
Trip Gheorghe (Emergency County Hospital,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Hasharon Hospital,
Zilahi Karoly (SCM Praxis, Bixad, România)
Tel Aviv, Israel)
Zeidman Aliza (Hasharon Hospital, Tel Aviv, Israel)
Horber Orsolya (SCM Praxis Bixad, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
ASSOCIATED EDITOR
College of Physicians Satu Mare
Satu Mare Association of Family Physicians
Satu Mare, 23 Eroilor Revolu iei Pl.
A liated with National Society of Family Medicine/
General Medicine
email: colmedsm@gmail.com
Satu Mare, UK 30 Bobocului St.
PARTNERSHIP
EXTERNAL PARTNERSHIP
Titu Maiorescu University, Bucharest
Vasile Goldiş
Hasharon Hospital,
Faculty of Medicine and Dental Medicine
Western University of Arad
Rabin Medical Center
67A Gheorghe Petraşcu St.
94 Revolutiei Blvd., Arad, Romania
A liated with Sackler School of Medicine,
Petah Tikva 49372, Israel
EDITORIAL OFFICE
23 Eroilor Revolu iei Pl., 440055, Satu Mare, Romania, Tel/Fax: 0040261-710456, 0040361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Journal included in e Schedule of Medical Publications of CMR, 10 credits CMR for subscribers
Indexed in Index Copernicus®, CNCS B+ Category, Code 944
Medical Connections/Conexiuni Medicale® is a trademark of College of Physicians Satu Mare and Satu Mare Association of Family Physicians
Printed at TIPOOFFSET, Fabricii st, No. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
SCIENTIFIC AND PEER REVIEW BOARD | COLECTIV ŞTIIN IFIC ŞI DE RECENZIE
Acad. Prof. Univ. as. Dr. Virgil Enătescu
Prof. Univ. Dr. Tuvia Hadar
(Emergency County Hospital, Satu Mare,
(Beilinson Hospital, Rabin Medical Center, Sackler
Romania)
Faculty of Medicine, Tel Aviv University, Israel)
Acad. Prof. Univ. Dr. Doina Onicescu
Prof. Univ. Dr. Gheorghe Manole
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Sorin Riga
Prof. Univ. Dr. Dorel Augustin Manu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Acad. Senior Scienti c Researcher Dr. Dan Riga
Prof. Univ. Dr. Dan Mănăstireanu
(Prof. Dr. Al. Obregia Clinic Hospital of Psychiatry,
(Titu Maiorescu University, Faculty of Medicine
Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Vasile Astărăstoae
Prof. Univ. Dr. Elena Moldoveanu
(Gr. T. Popa University of Medicine and Pharmacy,
(Titu Maiorescu University, Faculty of Medicine
Iaşi, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Rumelia Koren
Prof. Univ. Dr. Adriana Stănilă
(Hasharon Hospital, Rabin Medical Center, Sackler
(Victor Papilian Faculty of Medicine, Sibiu,
School of Medicine, Tel Aviv University, Israel)
Romania)
Prof. Univ. Dr. Petru Armeanu
Prof. Univ. Dr. Maria Lidia Nica Udangiu
(Titu Maiorescu University, Faculty of Medicine
(Titu Maiorescu University, Faculty of Medicine
and Dental Medicine, Bucharest, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Ilie Constantin
Prof. Univ. Dr. Dan Florin Ungureanu
(Victor Babeş University, Faculty of Medicine,
(Titu Maiorescu University, Faculty of Medicine
Timişoara, Romania)
and Dental Medicine, Bucharest, Romania)
Prof. Univ. Dr. Gheorghe Ionel Comşa
Conf. Univ. Dr. Ghinescu Minerva
(Ovidius University, Constan a, Romania)
(Titu Maiorescu University, Bucureşti, România)
Prof. Univ. Dr. Constantin Dumitru
Conf. Univ. Dr. Mircea Sorin Sabău
(Titu Maiorescu University, Faculty of Medicine
(University of Medicine and Pharmacy Târgu
and Dental Medicine, Bucharest, Romania)
Mureş, Romania)
Prof. Univ. Dr. Rivka Gal
Ş. L. Dr. Anca Ciurea
(Hasharon Hospital, Rabin Medical Center, Sackler
(Iuliu Ha ieganu University, Faculty of Medicine,
School of Medicine, Tel Aviv University, Israel)
Cluj Napoca, Romania)
Prof. Univ. Dr. Doina Lucia Ghergic
Ş. L. Dr. Virgil Radu Enătescu
(Titu Maiorescu University, Faculty of Medicine
(Eduard Pam l Universitary Clinic of Psychiatry,
and Dental Medicine, Bucharest, Romania)
Timişoara, Romania)
e Medical Connections/Conexiuni Medicale® is indexed in Journals Master List of Index Copernicus®
CNCS B+ Category, Code 944
© Copyright Medical Connections/Conexiuni Medicale, Satu Mare, 2014
No part of this publication may be reproduced, stored in a retrieval system or transmitted in any form or by any
means without prior permission in writing of Medical Connections/Conexiuni Medicale®. Permission is not
however required to copy abstracts of papers or of articles on condition that a full reference to the source is
shown. Correspondence regarding permission to reprint all or part of any article published in this journal
should be addressed to the Editor, e-mail: colmedsm@gmail.com
MEDICAL CONNECTIONS | CONEXIUNI MEDICALE®
EDITORI ADJUNC I
EDITOR ŞEF
Blaga Vasile (versiunea electronică)
Koren Rumelia
Andó Ottó (versiunea tipărită)
EDITOR ŞEF ADJUNCT
Oană Cristian Sever (editorialist)
Bumbulu Călin
Stăncioiu Tudor (Medicina Dentară)
COMITET EDITORIAL
Bauer Adalbert (SCM West Satu Mare, România)
Kesler Gavriel (Israel)
Bidilean Nicolae (Spital Jude ean de Urgen ă,
Kiss Ladislau (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Boros Melinda (Bucureşti, România)
Mihalca Man Sorina (Spital Jude ean de Urgen ă,
Borcean Gheorghe (Spital Municipal Caransebeş, România)
Satu Mare, România)
Brândeu Ioan (Spital Jude ean de Urgen ă,
Neumann Gad (Spital Hasharon, Tel Aviv, Israel)
Satu Mare, România)
Negru Alina (SCM Satu Mare, România)
Cârstea Constantin (CMI Braşov, România)
Rath-Wolfson Lea (Spital Hasharon, Tel Aviv, Israel)
Cojocaru Manole (Universitatea Titu Maiorescu,
Rădulescu Viorel (CMI Olt, România)
Bucureşti, România)
Roatiş Marius Dinu (Spital Jude ean de Urgen ă,
Comăneanu Raluca Monica (Universitatea Titu Maiorescu,
Satu Mare, România)
Bucureşti, România)
Rusu Cristian Bogdan (Spital Jude ean de Urgen ă,
Cornean-Santa Corina (Spital Jude ean de Urgen ă,
Satu Mare, România)
Satu Mare, România)
Shvero Kesler Dana (Universitatea Hadassa,
Feciche Bogdan (Spital Jude ean de Urgen ă,
Ierusalim, Israel)
Satu Mare, România)
Trip Gheorghe (Spital Jude ean de Urgen ă,
Grosz Gyula (SCM West Satu Mare, România)
Satu Mare, România)
Gruzman Carlos (Spital Hasharon, Tel Aviv, Israel)
Zilahi Karoly (SCM Praxis, Bixad, România)
Horber Orsolya (SCM Praxis Bixad, România)
Zeidman Aliza (Spital Hasharon, Tel Aviv, Israel)
Lup Liliana (Synevo Satu Mare, România)
Virag Tiberiu (CMI Satu Mare, România)
EDITOR
EDITOR ASOCIAT
Colegiul Medicilor Satu Mare
Asocia ia Medicilor de Familie Satu Mare
Satu Mare, P- a Eroilor Revolu iei nr.23
A liată la Societatea Na ională de Medicina Familiei/
Medicină Generală
email: colmedsm@gmail.com
Satu Mare, str. Bobocului UK 30
PARTENER
PARTENER EXTERN
Universitatea Titu Maiorescu Bucureşti
Universitatea de Vest Vasile Goldiş
Hasharon Hospital, Rabin Medical Center
Facultatea de Medicină şi Medicină Dentară
din Arad
A liat la Sackler School of Medicine,
str. Gheorghe Petraşcu 67A
94 Revolu iei Blvd., Arad, România
Universitatea Tel Aviv
7 Keren Kayemet St.,
Petah Tikva 49372, Israel
REDAC IA
P- a Eroilor Revolu iei nr 23, 440055, Satu Mare, Romania, Tel/Fax: 0261-710456, 0361-408164
ISSN online 2068 - 8369
ISSN 1843 - 9306
Revistă inclusă în Nomenclatorul Publica iilor Medicale ale CMR, 10 credite CMR pentru abona i
Indexare în Index Copernicus®, CNCS categoria B+, cod 944
Medical Connections/Conexiuni Medicale® este marcă înregistrată a Colegiului Medicilor Satu Mare şi a Asocia iei Medicilor de Familie Satu Mare
Tipărit la TIPOOFFSET, str. Fabricii, Nr. 93-103, Cluj Napoca, Tel.: 0040264-456071, Fax: 0040264-595711
Contents
EDITORIAL
7
ORIGINAL ARTICLES
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical
and Electrical Activity Using Ex-Vivo Rat Hearts
Mihai Mărginean, Alina Ardelean-Maghiar, Ovidiu Simion Cotoi, Gheorghe Bărbat, Marcel Perian
11
Histopathological Comparative Assessment of Osseointegration Processes of Titanium
and Zirconium Dental Implants in the Rabbit Femur
Bogdan A Bumbu, Bogdan Uivărășeanu, Adrian G Bumbu, Traian T Maghiar
19
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
Dănu Dejeu, Aurel Babeș
25
News in the Treatment of Hepatic Hydatid Cyst
Adela Camelia Nichita, Adrian Maghiar, Daniela Dinulescu, Teodor Traian Maghiar
35
Comparison Between the Classic Surgical Methods and the laparoscopic Ones
in the Benign Tubo-Ovarian Pathology
Nicolae Babău, Marius Sebastian Teodorescu
43
GENERAL REVIEW
Adoptive Cell Transfer - a New Hope for Metastatic Melanoma Patients. A Review
Golan Bubis, Călin Bumbulu , Lea Rath-Wolfson
55
Laparoscopic Treatment in Rectal Cancer. Where are we in 2014?
George Dejeu, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Marius S rlea, Codru a Macovei
59
Myocardial brosis a pathophysiological process in cardiac remodelling
Lala I. Radu, Maria Pușchi ă
63
CASE PRESENTATION
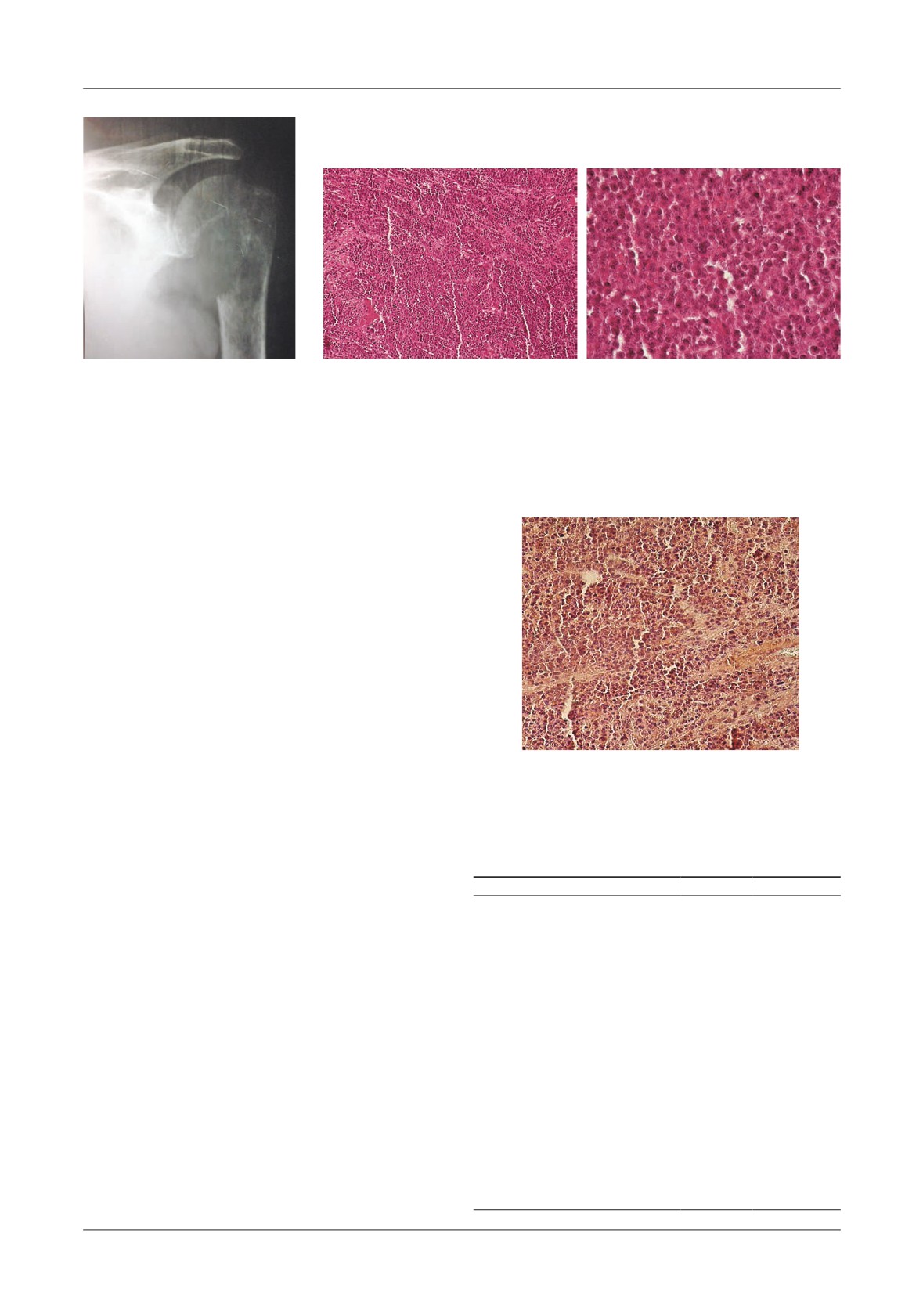
Primary Difuse Large B-Cell Lymphoma of the Humerus. Case Report and Review of Literature
Oana Pobirci, Elena Roșca, Dumitru Decebal Pobirci, Adela Nichita
69
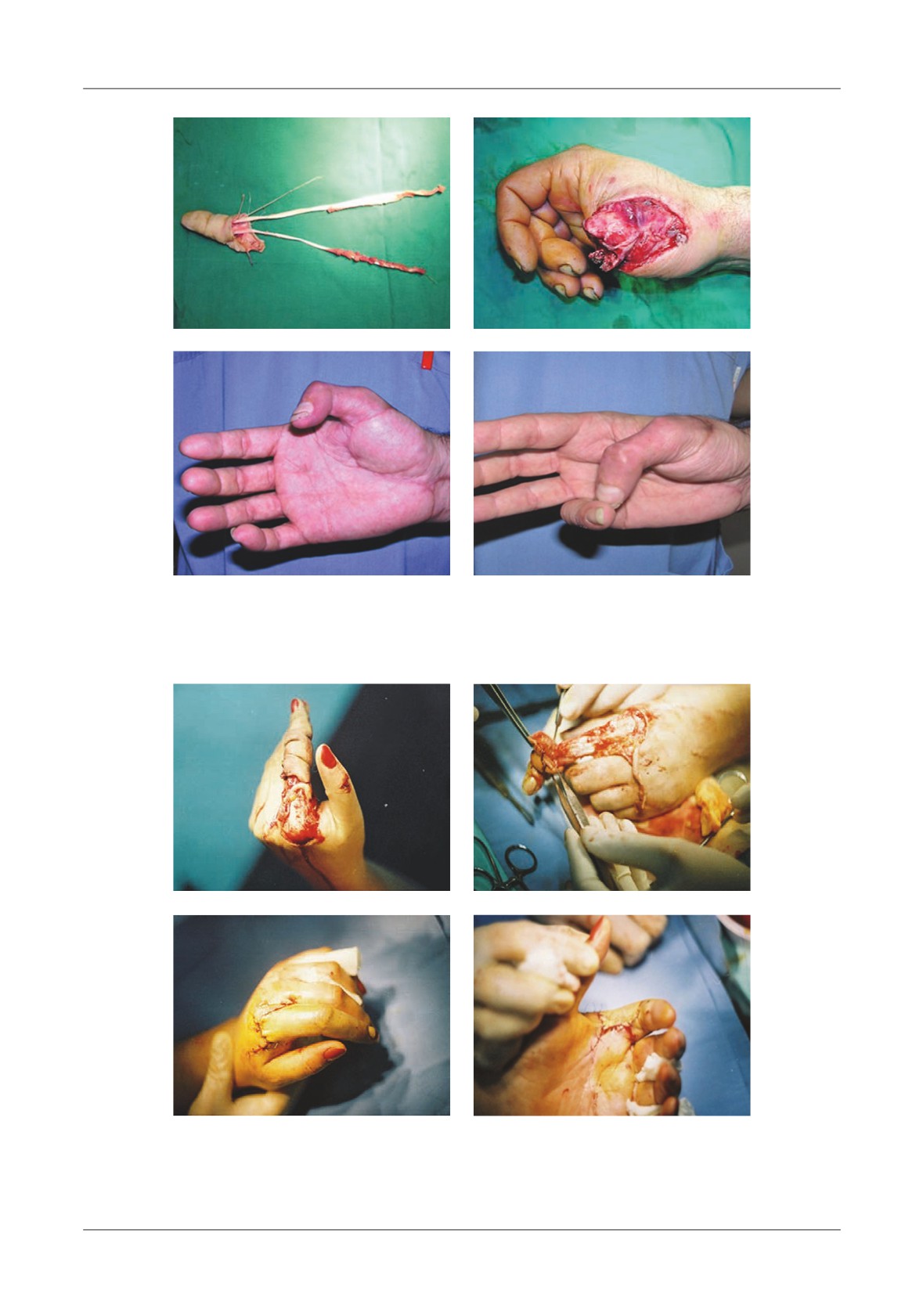
Replantation of Amputated Fingers after Ring Avulsion. Technical Considerations and Functional
Prognosis Results
Doina Prisecari, Dragoș Zam rescu, Șerban-Arghir Popescu, Ioan Lascar, Alisa Zisman, Alexei Prisecari
73
HISTORY OF MEDICINE
Constantin Stanca (1889-1969) - a Prestigious Gynecologist and Oncologist of the 20th Century
Cristian D. Barsu
79
GUIDANCE FOR AUTHORS
83
Cuprins
EDITORIAL
87
ARTICOLE ORIGINALE
Evaluarea precondi ionării ischemice miocardice cuanti când activitatea electrică și mecanică
post-ischemică folosind corduri de șobolan ex-vivo
Mihai Mărginean, Alina Ardelean-Maghiar, Ovidiu Simion Cotoi, Gheorghe Bărbat, Marcel Perian
91
Evaluarea histopatologică comparativă a proceselor de osteointegrare a implanturilor de titan
și zirconiu în osul femural la iepure
Bogdan A Bumbu, Bogdan Uivărășeanu, Adrian G Bumbu, Traian T Maghiar
99
Urmărirea cazurilor de abdomen acut la pacien ii diabetici comparativ cu cei nondiabetici
Dănu Dejeu, Aurel Babeș
105
Actualită i în tratamentul chistului hidatic hepatic
Adela Camelia Nichita, Adrian Maghiar, Daniela Dinulescu, Teodor Traian Maghiar
115
Compara ie între metodele chirurgicale clasice și laparoscopice în patologia benignă tubo-ovariană
Nicolae Babău, Marius Sebastian Teodorescu
123
REVISTĂ GENERALĂ
Transferul de celule de adop ie - o nouă speran ă pentru pacien ii cu melanom metastazat.
O revistă a literaturii
Golan Bubis, Călin Bumbulu , Lea Rath-Wolfson
135
Tratamentul laparoscopic în cancerul rectal. Unde suntem în 2014?
George Dejeu, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Marius S rlea, Codru a Macovei
139
Fibroza miocardică, proces ziopatologic în remodelarea cardiacă
Lala I. Radu, Maria Pușchi ă
143
PREZENTARE DE CAZ
Limfom primar difuz cu celule tip-B mari al humerusului. Prezentare de caz și revistă a literaturii
Oana Pobirci, Elena Roșca, Dumitru Decebal Pobirci, Adela Nichita
149
Replantarea degetelor amputate prin mecanisme de avulsie-torsiune. Considera ii tehnice
și rezultate func ionale
Doina Prisecari, Dragoș Zam rescu, Șerban-Arghir Popescu, Ioan Lascar, Alisa Zisman, Alexei Prisecari ... 153
ISTORIA MEDICINEI
Constantin Stanca (1889-1969) - un ginecolog și oncolog prestigios al secolului al XX-lea
Cristian D. Barsu
159
STANDARDE DE PUBLICARE
163
Colegiul Medicilor
Satu Mare
Colegiul Medicilor Satu Mare este o persoană juridică autonomă, neguvernamentală,
apolitică şi fără scop patrimonial. Este într-o largă accep iune o organiza ie profesională
liberală şi reuneşte peste 626 de medici.
Colegiul Medicilor Satu Mare crede că poate reuşi urmând trei principii: să vorbească doar
când are ceva important de spus, să nu critice până când nu are solu ii şi să nu propună decât
solu ii rezultate din sfatul colectiv. For a Colegiului Medicilor constă în prezentarea în fa a
societă ii ca o voce autentică, permanent validată, a tuturor membrilor săi.
Satu Mare College of Physicians is an autonomous legal entity, non-governamental, apolitical
and non-pro t. In a widley acception it is a liberal professional organization and brings
together over 626 doctors.
Satu Mare College of Physicians believes it can succeed by following three principles: to
speak only when he has something important to say, to make no critics until he has solutions
and to propose only solutions resulted from a of collective advice. e force of Physicians
College consist in showing in front of the society an authentic voice, always validated, from
all its members.
Eroilor Revolu iei Pl. no.23, 440055 Satu Mare, Romania.
Tel./Fax: +40-261-710456, +40-361-408164, e-mail: colmedsm@gmail.com
EDITORIAL
e eleventh edition of Satu Mare Medical Days,
dr. Levai Lehar, dr. Pal Bagosi, dr. Carmen Caprar, dr.
organized by the Satu Mare College of Physicians and
Marta Csik Maticu, dr. Olimpia Ster, dr. Irina Csutak,
the Association of Family Physicians Satu Mare, in
dr. N. Feraru, Department of Ophthalmology, from
partnership with Rabin Medical Center, a liated to the
Satu Mare Emergency County Hospital and „Refractive
Sakler School of Medicine, Tel Aviv University (Israel),
Surgery to Reduce Diopters”, authors: dr. Levai Lehar, dr.
Faculty of Medicine and Dentistry, Titu Maiorescu
Orsolya Dohi, dr. D. Aracs, Dr. Angela Malachi, dr.
University of Bucharest, and Vasile Goldis Western
Livia Olah, from Department of Ophthalmology, the
University of Arad, was held between 2nd and 4th October
Satu Mare Emergency County Hospital. Dr. Cristina
2014.
e President of the Scienti c Committee, as
Maria Andrei, Vascular Surgery Specialist Physician,
every year, was Mrs. Professor Dr. Rumelia Koren from
Satu Mare County Hospital, presented her works: „ e
the University of Tel Aviv. Special guests were: Acad.
Importance of Vascular Surgery Department in Satu Mare
Prof. Univ. Dr. Virgil Enătescu, and Dr. Ileana Filipescu
Emergency County Hospital” and „Infrapopliteal Bypass in
from Rheumatology Clinic of Cluj Napoca.
Salvage of the Ischemic Lower Limb (Clinical Case)” the
e rst day,
ursday, October 2nd was opened by
last presentation having as co-author dr. Filip Dan, from
the President of Satu Mare College of Physicians, dr.
the Baia Mare County Hospital, the Department of
Călin Bumbulu , in the presence of representatives of
Interventional Cardiology. After the break, the works
state institutions and of professional associations: the
were resumed by the presentation of dr. Stelian Pop,
Prefect, dr. Eugeniu Avram, the Mayor of Satu Mare, dr.
Oncology and Hematology Senior Physician: „Treatment
Dorel Coica, the President of Satu Mare College of
Begins with the Pathologic Anatomy; From the Symptom to
Dentists, dr. Flaviu Simu, the Rector of Vasile Goldis
the System, for Quality of Medical Care”.
e following
Western University, Professor dr. Gavrilă Ardelean, the
works were presented by dr. Bogdan Feciche „Radical
manager of Satu Mare County Emergency Hospital Erika
Cystectomy with Ileal neobladder. Initial Experience”,
Venemozer, the President of Satu Mare Insurance House
authors: dr. Bogdan Feciche, dr. Dumitru Fanea, dr.
ec. Georgeta Pop, the Executive Director of Satu Mare
Lilian Gorbatai, dr. Cristian Rusu, dr. Neli Moroșanu,
County Health Department, dr. Dorina Dragos Guran.
dr. Vitalie Moroșanu, dr. Roxana Rugea, dr. Roxana
All representatives have expressed words of support and
Oltean, dr. Florian Vereş and
„Radical Retropubic
appreciation for the medical sta of Satu Mare County.
Prostatectomy”, authors: dr. Bogdan Feciche, dr. Cristian
e scienti c papers of the conference started with
Rusu, Dr. Nicolae Salageanu, dr. Lilian Gorbatai, dr.
„ yroid Gland Involvement in Advanced Laryngeal
Florian Vereș, dr. Vitalie Moroșanu, dr. Neli Moroșanu,
Cancer” of the authors: dr. Ohad Hilly, dr. Lea Rath-
dr. Roxana Rugea, dr. Nicolae Branişte, dr. Aurel Lupşa.
Wolfson, dr. Raanan Raz, dr. Yona Vaisbuch, dr. Yulia
Dr. Cristian Rusu presented the works
„Retrograde
Strenov, dr. Karl Segal, dr. Jacob Shvero, dr. Rumelia
Ureteroscopy - the Experience of the Department of Urology
Koren from Tel Aviv University, presented by Professor
from the Satu Mare Emergency County Hospital” having
dr. Rumelia Koren. en followed: „Re ux Disease in
as authors dr. Cristian Rusu, dr. Bogdan Feciche, dr.
Chronic In ammatory Laryngeal Pathology” of the
Lilian Gorbatai, dr. Nicolae Salageanu, dr. Nicolae
authors: dr. Cornean Iulia Corina, resident physician,
Branişte, dr. Traianela Ionescu, dr. Aurel Lupşa, dr. Neli
dr. Cornean Corina, ENT Senior Physician, Satu Mare
Moroșanu, dr. Vitalie Moroșanu, dr. Roxana Rugea and
County Hospital, presented by dr. Cornean Corina, and
„Laparoscopic Nephrectomy and Nephroureterectomy - e
two works presented by dr. Levai Lehar „Accident at
Experience of Satu Mare Medical Sta ”, authors: dr.
Work Tragically Started but with Happy Ending”, authors:
Cristian Rusu, de. Bogdan Feciche, dr. Lilian Gorbatai,
7
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
dr. Nicolae Salageanu, dr. Tiberiu Botezan, dr. Florian
Journal, Report at Nine Years from the First Issue”, having
Vereș, dr. Alexandru Vasvari, dr. Nicolae Branişte, dr.
as authors: dr. Călin Bumbulu and dr. Vasile Blaga.
Traianela Ionescu, de. Aurel Lupşa, dr. Neli Moroșanu,
After the break followed „Quantifying the E ectiveness of
dr. Vitalie Moroșanu, dr. Roxana Rugea. „Evolution of
Biological
erapy Given to Patients with Active
the Notes and Medical Records. Historical Background”
Rheumatoid Arthritis” of the authors dr. Ileana Filipescu,
having as authors dr. Orsolya Horber and dr. Karoly
dr. Maria Deac, dr. Simona Rednic from the Clinic of
Zilahi, Family Medicine Senior Physicians, was
Rheumatology,
„Iuliu Ha ieganu” University of
presented by dr. Orsolya Horber. en followed „ e
Medicine and Pharmacy, Cluj-Napoca, presented by dr.
Situation of the Treatment of Myocardial Infarction with
Ileana Filipescu.
en dr. Rumelia Koren presented the
ST-Segment Elevation (STEMI) in Satu Mare, in the Last
conference
„ e role of Dendritic Cells in
yroid
Ten Years” of the authors: dr. Ladislas Kiss, dr. Alina
Papillary Carcinoma” having as authors dr. Rumelia
Roatiş, dr. Loredana Vinkler, dr. Ioana unaș, dr.
Koren, dr. Ohad Hilly, dr. Lea Rath-Wolfson from the
Melinda Kurtinecz, dr. Carmen Șimon, dr. Victor
University of Tel Aviv. e presentations followed with
Orban, the Department of Cardiology, from Satu Mare
those of the Department of Gynecology from the Satu
County Hospital, presented by dr. Alina Roatiş.
e
Mare County Hospital: „TB in Con nement after Birth”,
conference
„Expression of Matrix Metalloproteinases-1
authors: dr. Viorica Varodi, dr. Gra ian Tudor u uraş,
(MMPs-1) in Well-Di erentiated
yroid Carcinoma
dr. Cornel Căpitan, Dr. Liviu Ardelean, dr. Mircea
(WDTC) with Laryngo-Tracheal Invasion” presented by
Dragoș, dr. Vasile Matiz, dr. Ștefan Pop, dr. Carmen
dr. Rumelia Koren had as authors: dr. Aviram Mizrachi,
Derşidan, dr. Bogdan Fărcaș, dr. Manuela Heim, dr.
dr. Lea Rath-Wolfson, dr. Tuvia Hadar, dr. Eitan Yaniv,
Lucian Radu Costin, dr. Anca Dăscălescu-Bogdan,
dr. Sara Morgenstern, dr. Jacob Shvero, dr. Rumelia
presented by dr. Viorica Varodi, and
„Case Report:
Koren from the University of Tel Aviv. First day of the
Ectopic Pregnancy-Internal Hernia”, authors: dr. Gra ian
manifestation was closed by „ e Physician as Public
Tudor u uraş, dr. Viorica Varodi, dr. Cornel Căpitan,
Servant. A political vision or politicising?” presented by
dr. Liviu Ardelean, dr. Mircea Dragoș, dr. Vasile Matiz,
dr. Călin Bumbulu , having as authors dr. Călin
dr. Ștefan Pop, dr. Carmen Derşidan, dr. Bogdan Fărcaș,
Bumbulu , Family Medicine Senior Physician, dr. Alina
dr. Manuela Heim, dr. Lucian Radu Costin, dr. Anca
Negru, Family Medicine Senior Physician, dr. Nicolae
Dăscălescu-Bogdan, dr. Vitalie Moroșanu, dr. Bogdan
Sebastian Balaj, Family Medicine Specialist Physician,
unaș, and „Diagnostic and
erapeutic Hysteroscopy”,
dr. Vasile Blaga, Family Medicine Senior Physician.
authors: dr. Anca Dăscălescu-Bogdan, dr. Viorica
We emphasize the value of the works presented at
Varodi, dr. Cornel Căpitan, Dr. Liviu Ardelean, dr.
the Satu Mare Medical Days, one of dr. Lehar Levai’s
Mircea Dragoș, dr. Vasile Matiz, dr. Ștefan Pop, dr.
presentations „Accident at Work Tragically Started but
Carmen Derşidan, dr. Bogdan Fărcaș, dr. Manuela
with Happy Ending” obtained, short after our
Heim, dr. Lucian Radu Costin, the last two being
manifestation, the rst prize at the National Conference
presented by dr. Anca Dăscălescu-Bogdan. Two works:
of Ophthalmology.
”Endoscopic Variceal Ligation - Life Saving Intervention”
e second day started with the works: „Prevention
and „Removal of Esofagial Foreign Body
- Emergency
of the Borreliosis” and
„ e Ticks” presented by dr.
Endoscopic Intervention” have been authored by dr.
Margareta Fulop, Infectious Diseases Senior Physician,
Marian Bogdan Zota, Gastroenterology Senior
from Satu Mare County Hospital. e works continued
Physician, from Satu Mare County Hospital.
e
with
„Stepwise Treatment of Pain” presented by dr.
second day was concluded by dr. Călin Bumbulu with
Loredana Aracs Tamas, having as authors dr. Loredana
„Migration of Doctors from Romania”.
Aracs Tamas, dr. Stelian Pop, dr. Bușilă Emilian, dr.
Last day of the Satu Mare Medical Days was splitted
Susana Szentesi, the Department of Medical Oncology
in two sections: Medical History and Medicine and
of the Satu Mare Emergency County Hospital. en
Art. e Section of Medical History has already become
followed two works:
„Functional Reconstruction of
a tradition at Satu Mare Medical Days, and included:
Postexcisional Defects of Upper and Lower Eyelid with
„Two Communications Regarding the Activity of dr. Luko
Muscle Flaps from Vecinity” and „Urethral Reconstruction
Bela” of the authors: dr. Alina Negru, dr. Călin
in Two Steps of Penile Hypospadias Using Buccal Mucosa
Bumbulut, dr. Sebastian Balaj, dr. Vasile Blaga, „ e
and Vascularized Flaps of Penile Dartos. Correction of the
History of Hospital Institution of Tăşnad” with the
Pseudo stulae” of dr. Marius Dinu Roatiş, Plastic Surgery
authors: dr. Zoltan Vass, dr. Otto Schmidt, „Medical
Senior Physician, from Satu Mare County Hospital. Dr.
Histories in Memoirs of Queen Marie of Romania, part II”
Călin Bumbulu presented
„Medical Connections
by authors: dr. Călin Bumbulu , stud. Andrei Bumbulu ,
8
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
EDITORIAL
Prof. dr. Rumelia Koren. Between sections, dr. Koren
Israel. Section was completed by „ e Permanent Art
Rumelia togheter with dr. Călin Bumbulu presented
Exhibition from Beilinson Hospital, Petah Tikva, Israel”
the conference „Guidelines for Writing a Scienti c Paper”.
having as authors by Prof. dr. Rumelia Koren, and dr.
en followed the Section Medicine and Art with
Călin Bumbulu .
„Marfan Syndrome in Painting” with the authors: dr.
e audience has appointed by vote the winners of
Călin Bumbulu , dr. Alina Negru, Prof. dr. Rumelia
the ve Awards of Excellence: dr. Viorica Varodi, dr.
Koren, „Langdon-Down Syndrome in Painting” authors:
Marius Roatiş, dr. Marian Bogdan Zota, dr. Levai Lehar
dr. Alina Negru, dr. Călin Bumbulu , Prof. dr. Rumelia
and dr. Margareta Fulop.
Koren, „Representation of Polio Sequelae in Art” authors:
Eleventh edition of the Satu Mare Days Medical has
Prof. dr. Rumelia Koren, dr. Alina Negru, dr. Călin
presented 40 works of 90 authors, in the three days have
Bumbulu , „Paintings of a Case of Obesity from the
participated
305 registered doctors, the discussions
Eighteenth Century, Probably due to Prader-Willi
occasioned being intense, particularly during the second
Syndrome” authors: dr. Călin Bumbulu , dr. Alina
day, involving scienti c issues, but also administrative
Negru, Prof. dr. Rumelia Koren, „ e Cabinet of Art and
organization of some departments of Satu Mare County
Curiosities at Ambras Castle, Austria” authors: Prof. dr.
Hospital. We mention the di culties created by the
Rumelia Koren, dr. Călin Bumbulu , stud. Andrei
closure of Satu Mare airport, even during the event,
Bumbulu , dr. Alina Negru, „Imagine all Images Catching
restricting thus the participation of colleagues from
Live”, authors: dr. Gabrieli Selma, dr. Benzaquen Oshri,
Bucharest and abroad.
from the Department of Imagistic, Hasharon Hospital,
We hope that the next edition, the twelfth, in 2015
Rabin Medical Center, Petah Tikva, a liated with
in the rst week of October, will be held under better
Sackler School of Medicine, University of Tel-Aviv,
auspices.
Assistant Editor in Chief: Călin Bumbulu
9
Medical Connections/Conexiuni Medicale
Conflict-of-Interest Statement
Medical Connections/Conexiuni Medicale (Med Con) requires all authors and reviewers to declare any
con icts of interest that may be inherent in their submissions.
Con ict of interest for a given manuscript exists when a participant in the peer review and publication
process-author, reviewer, or editor - has ties to activities that could inappropriately in uence his or her
judgment, whether or not judgment is in fact a ected.
Financial relationships with industry, for example, through employment, consultancies, stock
ownership, honoraria, expert testimony, either directly or through immediate family, are usually considered
to be the most important con icts of interest. However, con icts can occur for other reasons, such as
personal relationships, academic competition, and intellectual passion.
Public trust in the peer review process and the credibility of published articles depend in part on how
well con ict of interest is handled during writing, peer review, and editorial decision making. Bias can
often be identi ed and eliminated by careful attention to the scienti c methods and conclusions of the
work. Financial relationships and their e ects are less easily detected than other con icts of interest.
Participants in peer review and publication should disclose their con icting interests, and the information
should be made available so that others can judge their e ects for themselves.
Authors: When they submit a manuscript, whether an article or a letter, authors are responsible for
recognizing and disclosing nancial and other con icts of interest that might bias their work. ey should
acknowledge in the manuscript all nancial support for the work and other nancial or personal
connections to the work.
Reviewers: External peer reviewers should disclose to editors any con icts of interest that could bias
their opinions of the manuscript, and they should disqualify themselves from reviewing speci c
manuscripts if they believe it appropriate. e editors must be made aware of reviewers’ con icts of interest
to interpret the reviews and judge for themselves whether the reviewer should be disquali ed. Reviewers
should not use knowledge of the work, before its publication, to further their own interests.
Manuscript Title: ___________________________________________________________
I declare no con ict of interest
I declare the following potential con ict of interest:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Name
Signature/Date
Please fax or mail this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
Mail: colmedsm@gmail.com
ORIGINAL ARTICLES
EVALUATING MYOCARDIAL ISCHEMIC PRECONDITIONING BY
QUANTIFYING POST ISCHEMIC MECHANICAL AND ELECTRICAL
ACTIVITY USING EX VIVO RAT HEARTS
Mihai Mărginean1,4, Alina Ardelean-Maghiar2,5, Ovidiu Simion Cotoi3, Gheorghe Bărbat1, Marcel Perian1
Departments of 1Physiology, 2Laboratory Medicine Department, 3Cell and Molecular Biology, UMF Târgu-Mureș, and
4Departments of Anaesthesia and Intensive Care, and 5Clinical Laboratory, Military Emergency Hospital “Dr. Constantin
Papilian”, Cluj-Napoca, Romania
Address for correspondence:
Mărginean Mihai
18 Ana Aslan St., Cluj-Napoca, Cluj, Romania
Tel: +4 0754700271
E-mail: marginean.m@gmail.com
Received: 23.07.2014
Accepted: 15.09.2014
Med Con October 2014, Vol 9, No 3, 11-17
Abstract
recorded. At the end of the experimental protocol the
atria were removed and the ventricular myocardium was
Background: After discovering the preconditioning
submersed in Formaldehyde solution. Histology studies
e ect of ischemia and its protection against subsequent
were then performed using haematoxylin and eosin
ischemic injury, researchers have focused on better
staining.
understanding of the molecular pathways involved.
Results: Regarding the persistence of the hearts
During our experiment we tried to obtain data about
mechanical activity we did not nd a signi cant
how the electrical and mechanical activity of ex-vivo
di erence between the two groups (p=0.08). e period
hearts is a ected by a single short cycle of ischemia/
in which the hearts maintained a measurable electric
reperfusion.
activity after the prolonged ischemic insult di ered
Material and Methods: We used 30 adult Wistar
signi cantly (p=0.01). After the nal ischemic period
rats that were randomized in two groups: ischemic
and the restoration of perfusion, we recorded no further
preconditioning group (IPC, n=15) and control group
mechanical activity in any study group, but
11
(C, n=15). After proper anaesthesia (with Ketamine and
preparations (out of 15) from the IPC group regained
Xylazine) and anticoagulation (unfractionated Heparin)
their electrical activity which further lasted for approx.
hearts were excised and retrograde coronary perfusion
25 minutes.
was started using a Langendor device. Following a
Conclusions: Preconditioning ex-vivo rat hearts
period of stabilization, all hearts in the IPC group were
with a single ischemia/reperfusion cycle will result in a
subjected to a preconditioning protocol consisting of 5
more persistent electrical activity during subsequent
minutes of ischemia and 5 minutes of reperfusion before
sustained ischemia compared to non-preconditioned
a sustained 30 minute period of ischemia. e control
hearts, whereas the mechanical activity does not seem to
group only received the 30 minutes period of ischemic
be signi cantly in uenced by ischemic preconditioning.
injury. During the entire experiment heart rate, one-
Keywords: Ischemic Preconditioning, Rats, Wistar,
lead ECG and left ventricular pressure were continuously Myocardial Infarction
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
11
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Introduction
transition pore
(mPTP) [10]. e survivor activating
factor enhancement (SAFE) pathway which involves the
In 1986 Murry et al. [1] discovered that brief periods
TNFα and the signal transducer and activator of
of myocardial ischemia had the unexpected and
transcription-3 (STAT-3) [11], also leads to inhibition
paradoxical e ect of reducing the infarct size caused by
of the mPTP opening. e mPTP is the main e ectors of
circum ex coronary artery occlusion with up to 75%.
preconditioning [12]. Its opening causes the shutdown of
He used four cycles of intermittent occlusion/reperfusion
ATP production, mitochondrial swelling, and likely
lasting ve minutes each. is ability of the myocardium
cell-membrane rupture [13]. Other kinases are activated
to tolerate sustained ischemia after short episodes of
such as the protein kinase C [14] and the protein kinase
ischemia-reperfusion was named ischemic preconditioning
G [15], and are responsible for the activation of
(IPC). e powerful cardioprotective phenomenon was
mitochondrial ATP-dependent potassium channels
found to be present in all studied species. During IPC,
(mKATP) which are also likely e ectors of ischemic
the protective e ect has two phases.
e rst phase of
preconditioning [16,17].
protection begins immediately after the preconditioning
ese complex intracellular pathways raise a
trigger and lasts for 2-4 hours.
is is termed classical
number of questions that still remain unanswered even
ischemic preconditioning. A delayed phase of protection,
after decades of dedicated research.
referred to as the second window of protection (SWOP),
Our objective during this experiment was to provide
begins after 12-24 hours and lasts 2-3 days [2]. Ischemic
additional data about the interval of time until loss of
preconditioning involves several factors that are usually
electrical and mechanical activity following an ischemic
divided into three groups: triggers, mediators, and e ectors.
insult using a single cycle of ischemia/reperfusion.
e signalling pathways are complex and not yet fully
understood. Brief episodes of ischemia are causing the
Material and Methods
release of initiating factors such as adenosine, bradykinin,
and endorphins [3,4] (Figure 1).
is study was conducted in the Cardiovascular
During the rst phase, these initiators bind to their
Physiology Compartment (Department of Physiology)
speci c receptors coupled to G proteins resulting in
at the University of Medicine and Pharmacy in Târgu-
message transduction. Two signalling pathways have
Mureș. e experiment was designed to comply with
been identi ed.
e Reperfusion-Induced Salvage
European Union directives regarding the protection of
Kinase
(RISK) pathway
[5],
involves
the
animals used for scienti c purposes.
Phosphatidylinositol
3-Kinase (PI3-Kinase)
[6,7] the
We used 30 adult (5-8 months old) Wistar rats
protein kinase Akt
[8], and the extracellular signal-
housed in a temperature controlled environment and fed
regulated kinase ½ (ERK ½) [9]. ese kinases activate
under standard conditions (ad libitum standard rodent
glycogen synthetase kinase 3b (GSK-3b), which leads to
chow and water) with a body mass between 250g and
inhibiting the opening of the mitochondrial permeability
350g. ey were randomized in two groups: ischemic
preconditioning group (IPC, n=15) and control group
(C, n=15).
e animals were anaesthetized using
intraperitoneal Ketamine 100 µg/g and Xylazine 10 µg/g
[18]. A 2-3 cm mid-line abdominal incision was made,
intraperitoneal content was retracted and the left renal
vein was located. We administered 50 IU/100mg Sodic
Heparin IV (by direct puncture of the renal vein) [19].
After obtaining e cient anticoagulation
(spontaneous
di use bleeding at the skin incision site is noted) the
initial incision was extended both left and right and access
to the diaphragm muscle was assured. e diaphragm was
then cut and retracted so that the heart was visible. e
pericardial sack was opened and the heart was carefully
excised cutting the descendant aorta below the aortic arch
and submersed in a 4°C Krebs-Henseleit (K-H) bu er
solution [20].
is bu er solution was prepared before
every experimental session following a standard recipe
Figure 1. Ischemic preconditioning pathways
[19,21,22] and used only for a maximum period of 24
12
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
hours. Time elapsed from the diaphragm muscle incision
e software that we used for reading and interpreting
(which caused ine cient spontaneous breathing) until
the ECG signal also allows for time measurements. By
mounting the heart on the Langendor device and
knowing the exact time between two R-waves we were
retrograde myocardial perfusion was kept under
3
able to determine the heart rate (HR=1000/t(msec)x60).
minutes. e K-H bu er was continuously oxygenated
Mechanical activity of the heart was evaluated using
and perfused at a constant pressure (75 mmHg) and
a pressure transducer connected to a water- lled balloon
temperature
(37°C). After myocardial perfusion was
inserted in the left ventricle. Pressure recordings and
started, an incision through the left atrium wall was made
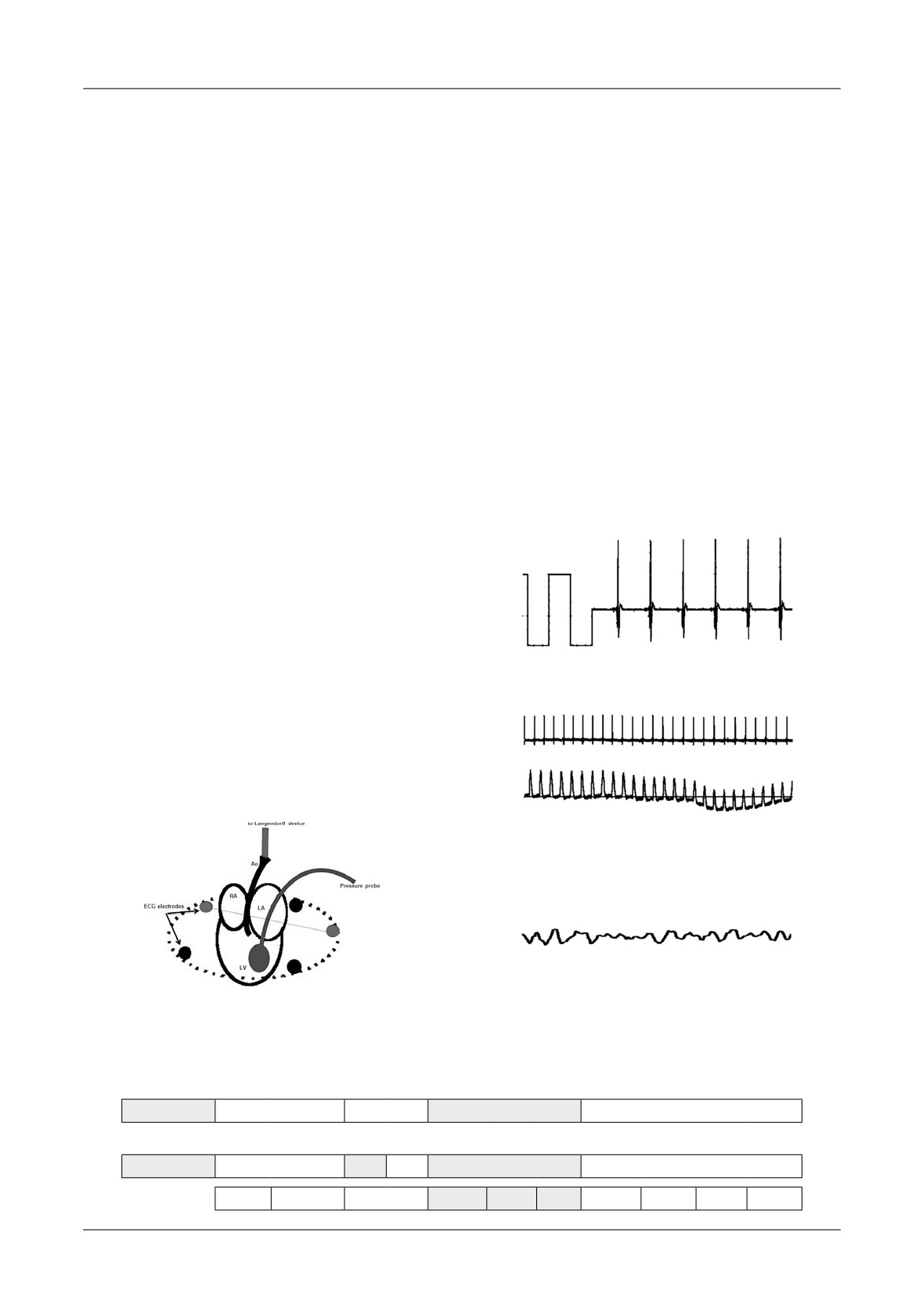
ECG were shown simultaneously (Figure 4).
and a pressure probe was advanced inside the left ventricle.
Figure 4. ECG ( rst trend) and LV pressure (second
A stabilizing period of 20 minutes followed at the end of
trend). Recorded during the stabilizing period (minutes
which all hearts needed to have a normal contraction rate
0-20). (HR=178 b/min)
and a stable rhythm [19]. For the IPC group, after this
One-lead ECG and LV pressure curves were recorded
initial period of stabilization, we induced a 5 minute
continuously until both electrical and mechanical
period of ischemia
(by stopping the K-H perfusion)
activity of the heart ceased. Even if this happened a few
followed by
5 minutes of reperfusion and then a
minutes after the beginning of the long ischemic injury
prolonged ischemia of 30 minutes. e control group
(minutes 30-60 - Table I) the reperfusion was allowed to
only received the
30 minutes ischemia period. After
continue for 40 minutes (minutes 60-100 - Table I) [1].
words a mandatory reperfusion period of 40 minutes was
For this study we did not perform any morphology
maintained so that ischemia-related metabolites could be
analysis of the electrical rhythm. Any type of rhythm
washed-out and subsequent cell injury avoided.
e
summary of the protocol is shown in Table I.
e electrical activity was recorded using two electrodes
from an array of ve that were placed around the heart.
After successful cannulation of the aorta and positioning of
the pressure probe inside the left ventricle, so that the
position of the heart became xed, we chose one electrode
near the right atrium and the second near the left atrium so
Figure 3. Calibration of ECG using a 1mV
that a DI-like lead was obtained (Figure 2).
electrical signal
Our ECG recording device allowed us to switch
between di erent electrodes as needed. e amplitude of
the recorded signal was calibrated using an initial 1mV
electrical current, as previously described [23] (Figure 3).
Figure 4. ECG ( rst trend) and LV pressure
(second trend). Recorded during the stabilizing
period (minutes 0-20). (HR=178 b/min)
Figure 5. Ventricular brillation. Subject
from C group. Recorded during the 30
Figure 2. ECG electrodes positioning
minutes ischemia
Table I. Timing protocol used
20 min
10 min
30 min
40 min
CONTROL
STABILIZATION
monitoring
ISCHAEMIA
REPERFUSION
20 min
5
5
30 min
40 min
IPC
STABILIZATION
I
R
ISCHAEMIA
REPERFUSION
minutes
10
20
30
40
50
60
70
80
90
100
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
13
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
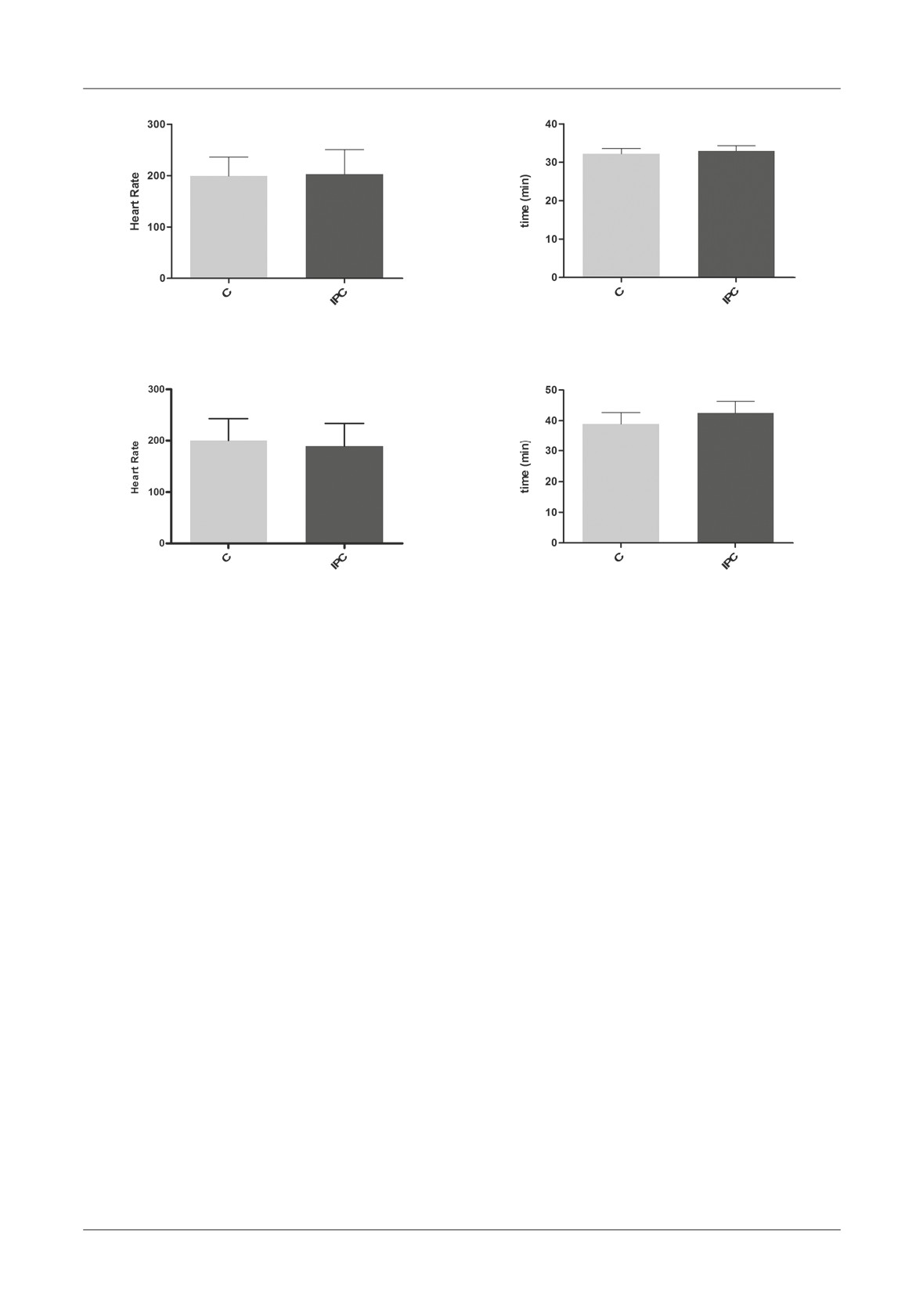
Figure 6. Heart rate recorded in minute 20 of
Figure 8. Moment when mechanical activity
the preconditioning protocol (mean±SD),
of the LV ceases (Mean±SD). Time shown
p=0.83
from the beginning of the experimental
protocol, p=0.08
Figure 7. Heart rate recorded in minute 30 of
Figure 9. Moment when electrical activity
the preconditioning protocol (Mean±SD,)
ceases (Mean±SD). Time shown from the
p=0.49
beginning of the experimental protocol, p=0.01
(with the exception of ventricular brillation - Figure 5)
When comparing the HR in minute 30 (after the
was considered electrical activity.
short ischemia/reperfusion cycle) we also found no
Mechanical activity was considered absent when no
statistical di erence (p=0.49) (Figure 7).
individual pressure wave was visible. After 100 minutes
e moment when the LV pressure probe ceased to
both atria were excised and the remaining ventricular
record mechanical activity did not di er signi cantly
myocardium was submersed in Formaldehyde (37%
(p=0.08). In both groups the mechanical activity was
solution). After at least 24 hours a basic histology study
lost after approx. 32-33 minutes (C, 1932±82 sec; IPC,
was performed using para n embedding and
1976±83 sec) (2-3 minutes after the induction of global
haematoxylin and eosin staining.
myocardial ischemia) (Figure 8).
Statistical analysis
Regarding the electrical activity we found a
We compared the time interval from the beginning
signi cant di erence between the two groups (p=0.01).
of the 30-minutes ischemia (minute 30, Figure 2) until
For the control group electrical impulses were recorded
all electrical and mechanical activity of the rat hearts
for approx. 38 minutes (C, 2332±225 sec.) and for the
ceased. Results are presented as mean±standard
IPC one for approx. 42 minutes (IPC, 2548±231 sec.)
deviation (SD) if not stated otherwise. A p value under
(Figure 9).
0.05 was considered signi cant. For statistical data
Time periods are considered from the beginning of
management we used commercially available software
the experimental protocol
(Table I). After the nal
(GraphPad Prism version
5.03 for Windows©,
ischemic period (minutes 30-60), when the perfusion
GraphPad Software, San Diego California USA).
was restarted, we recorded no further mechanical
activity in any of the groups. 11 preparations (out of 15)
Results
from the IPC group regained their electrical activity
which lasted approx. 25 minutes after the 30 minutes
e heart rates (HR) recorded in minute 20 (see
occlusion period (IPC, 1511±450 sec.).
Table I), at the end of the stabilizing period did not
e histology study o ered little additional data. It
di er signi cantly (p=0.83) (Figure 6).
did con rm the acute ischemic lesions in both groups
14
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
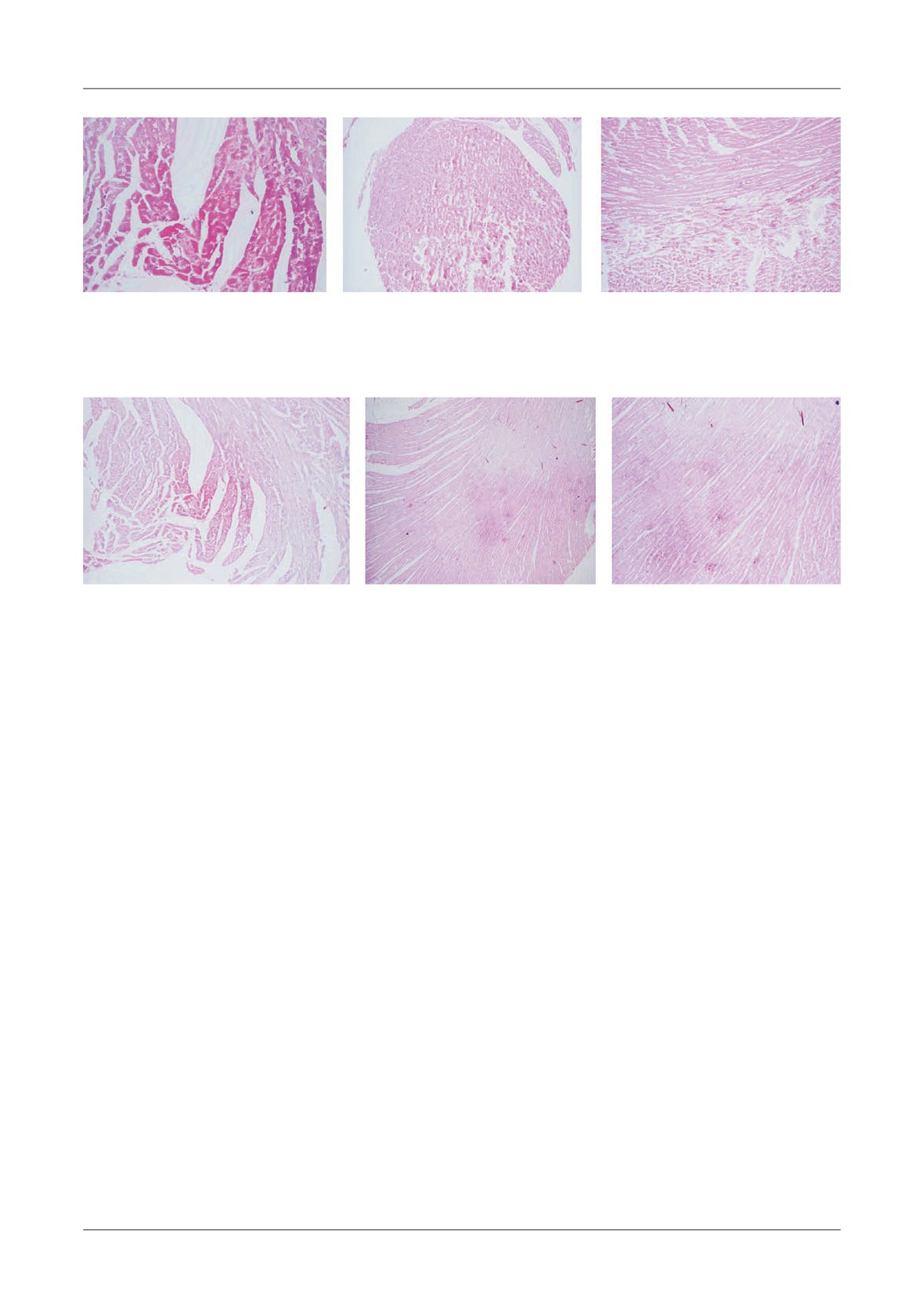
A
B
C
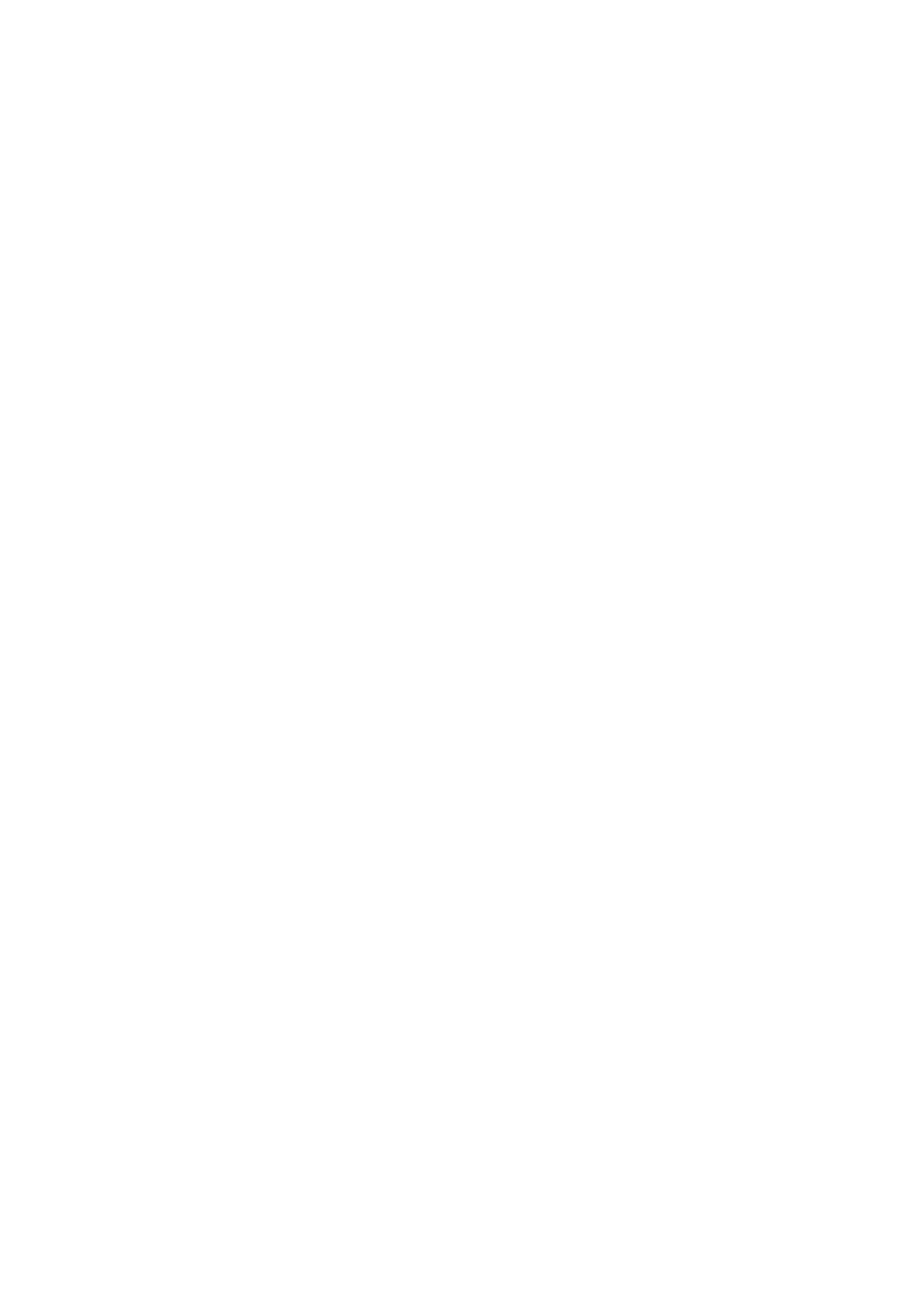
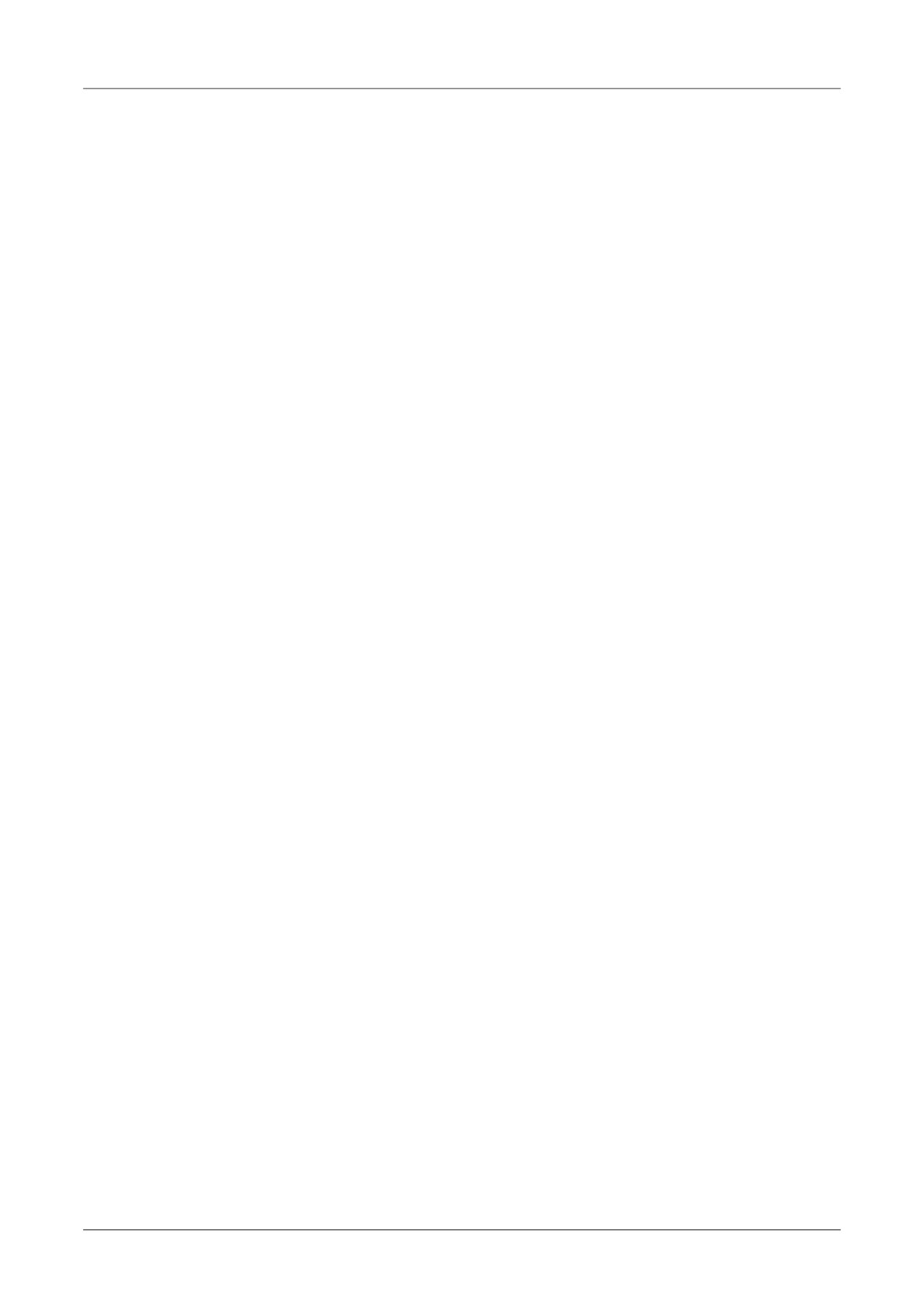
Figure 10. Group C. Ventricular myocardium. Acute ischemia. H&E staining. A - Myocardiocytes with
hypereosinophilic cytoplasm, dissipated striations, absence of nucleus 10x Ob. B - Ischemic spots visible at the level
of papillary muscles 4x Ob, C - Fragmentation of myocardial bres, hypereosinophilic cytoplasm,
focal disappearance of nuclei, 4x Ob.
A
B
C
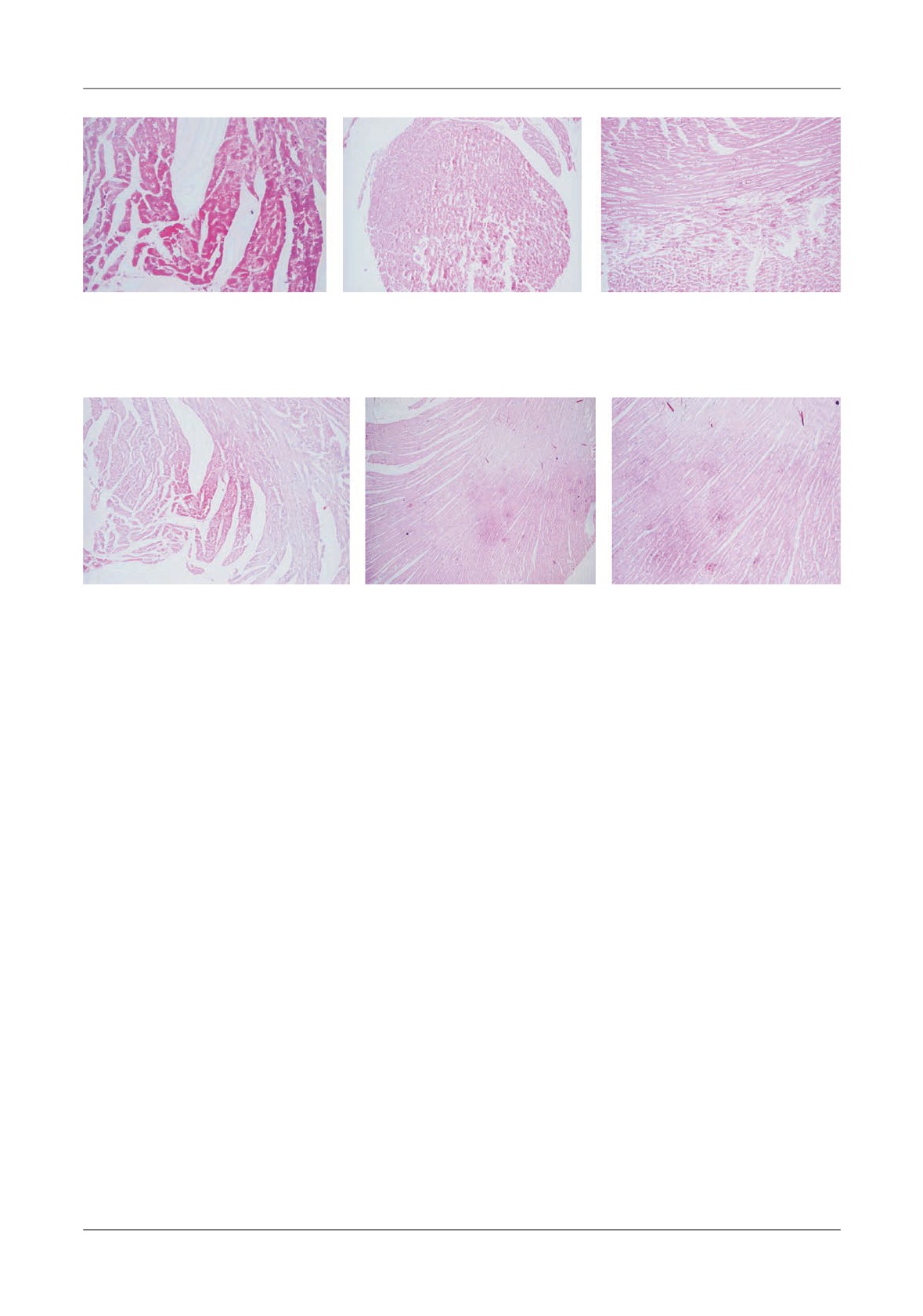
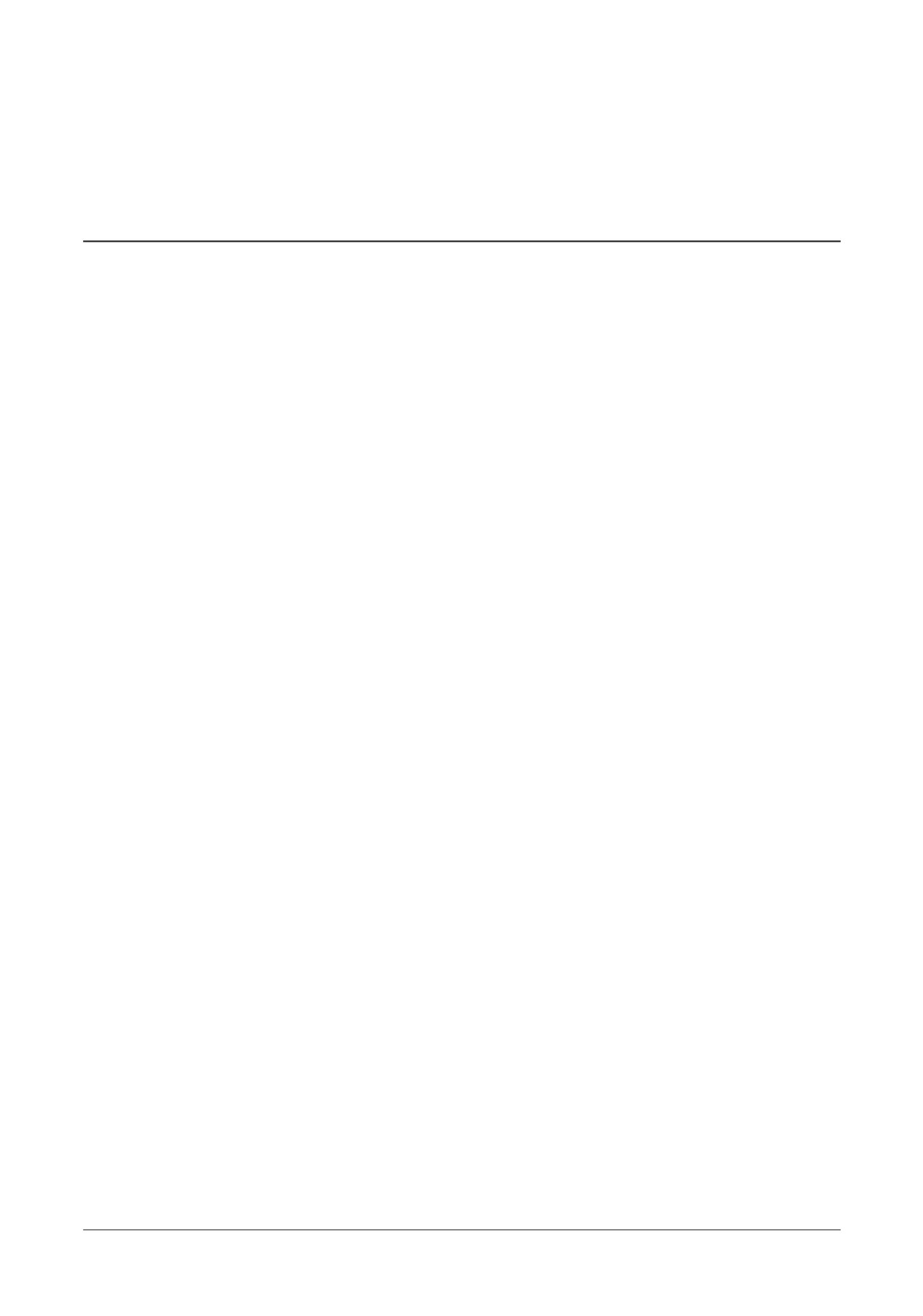
Figure 11. Group IPC. Ventricular myocardium. Acute ischemia. H&E staining A - Myocardiocytes with hypereosinophilic
cytoplasm, dissipated striations, absence of nucleus, 4x Ob. B - Spot visible through the ventricular wall, 2x Ob, C - Spot visible
through the ventricular wall, 4x Ob.
and showed more severe tissue alterations for the non-
rhythm, with the exception of ventricular brillation, as
preconditioned group (Figures 10 A,B,C), but exact
electrical activity.
quanti cation and statistical analysis was not possible
Regarding the LV pressure curve we were unable to
because of the di use lesions and intricate positioning
perform speci c analysis (like measuring the area-under-
of the a ected tissue alternating with normal one.
the-curve, AUC) because of our limited software
erefore no contour tracing could be employed. IPC
capabilities.
histological preparations are shown in Figures 11 A,B,C.
Our data indicate that during a period of sustained
ischemia, electrical activity persists longer in the
Discusssions
preconditioned group than in the control group, while
the mechanical activity does not seem to be in uenced
By recording the HR at the end of the stabilization
by preconditioning. e mechanism for this is probably
period (Figure 6) we tried to show that there was no
related to di erent ATP availability and usage. In both
di erence in the base-line status of the hearts before
groups, the amount of ATP generated in conditions of
ischemia/reperfusion cycle was employed for the IPC
severe ischemia is most probably insu cient to ensure
group. e statistical tests con rmed this (p=0.83) as
mechanical activity, hence, the lack of signi cant
was to be expected. But even after the 5 minutes I/R we
di erence between the two groups regarding this
did not nd any di erences regarding HR (Figure 7,
parameter. On the other hand, since ischemic
p=0.49). So the value of HR as a monitoring parameter
preconditioning seems to preserve better myocardial
will have to be increased in future experiments by
ATP levels
[25], the higher amount of ATP in
adding additional parameters (like optical imaging [24]
preconditioned hearts could explain the longer
and/or markers of myocardial necrosis - e.g. cardiac
persistence of electrical activity in this group. Opening
troponin).
of IK-ATP channels in response to hypoxia-induced
As we did not perform any morphology analysis for
intracellular ATP increase might explain the acceleration
the ECG recordings, data about the exact type of
of phase 3 of the action potential observed in myocytes
rhythm is not available. We classi ed any type of
subjected to ischemic preconditioning. In turn, this
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
15
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
could decrease the time for Ca2+ in ow during the
ischemia or heat stress is associated with resistance to
plateau phase of the action potential via the L-type Ca2+
myocardial infarction. Circulation 1993;88(3):1264-
channels, thus preventing a pro-apoptotic Ca2+ overload
72.
[26,27] and explaining the longer persistence of
3.
Downey JM, Davis AM, Cohen M V. Signaling
electrical activity in the preconditioned group.
pathways in ischemic preconditioning. Heart Fail Rev
e histology studies were limited by the available
2007;12(3-4):181-8.
staining options. For future research we advice the use
4.
Cohen M V, Yang X-M, Liu GS, Heusch G, Downey
of redox indicators to correctly asses’ cellular respiration
JM. Acetylcholine, Bradykinin, Opioids, and
(e.g. 2,3,5-triphenyl-2H-tetrazolium chloride) and also
Phenylephrine,
but
not
Adenosine,
Trigger
measure the infarct size with the help of a software
Preconditioning by Generating Free Radicals and
application that could perform contour tracing [28,29].
Opening Mitochondrial KATP Channels. Circ Res
As described earlier, we were unable to perform this.
2001;89(3):273-8.
Another limitation of this study is related to the
5.
Hausenloy DJ, Tsang A, Yellon DM. e reperfusion
anaesthetic drugs. Even if it has been suggested that
injury salvage kinase pathway: a common target for both
Ketamine could reduce the ischemic preconditioning
ischemic preconditioning and post conditioning. Trends
e ect and even block it altogether
[30] we were
Cardiovasc Med 2005;15(2):69-75.
compelled to use Ketamine because no other accepted
6.
Qin Q, Downey JM, Cohen M V. Acetylcholine but
anaesthetic technique was available at that moment.
not adenosine triggers preconditioning through PI3-
On the other hand, for this experiment we used a
kinase and a tyrosine kinase. Am J Physiol Heart Circ
single cycle of ischemia/reperfusion in contrast to the
Physiol 2003;284(2):H727-34.
majority of published data in order to assess the e ect
7.
Tong H, Chen W, Steenbergen C, Murphy E. Ischemic
and its magnitude.
Preconditioning Activates Phosphatidylinositol-3-Kinase
Upstream of Protein Kinase C. Circ Res
Conclusion
2000;87(4):309-15.
8.
Krieg T, Qin Q, Philipp S. Acetylcholine and
We conclude that preconditioning ex-vivo rat hearts
bradykinin trigger preconditioning in the heart through
with a single ischemia/reperfusion cycle will result in a
a pathway that includes Akt and NOS. Am J Physiol
more persistent electrical activity during sustained
Heart Circ Physiol 2004;36688:2606-11.
ischemia compared to non-preconditioned hearts,
9.
Hausenloy DJ, Tsang A, Mocanu MM, Yellon DM.
whereas the mechanical activity does not seem to be
Ischemic preconditioning protects by activating
signi cantly in uenced by ischemic preconditioning.
prosurvival kinases at reperfusion. Am J Physiol Heart
Circ Physiol 2005;288(2):H971-6.
Acknowledgments
10.
Juhaszova M, Zorov DB, Kim SH, et al. Glycogen
is paper is partly supported by the Sectorial
synthase kinase-3beta mediates convergence of protection
Operational Programme Human Resources Development
signaling to inhibit the mitochondrial permeability
(SOP HRD), nanced from the European Social Fund and
transition pore. J Clin Invest 2004;113(11):1535-49.
by the Romanian Government under the contract number
11.
Suleman N, Somers S, Smith R, Opie LH, Lecour
POSDRU 80641.
SC. Dual activation of STAT-3 and Akt is required
is project was nanced by internal research grants at
during the trigger phase of ischemic preconditioning.
the University of Medicine and Pharmacy from Tîrgu
Cardiovasc Res 2008;79(1):127-33.
Mureș, Romania. (CIGCS 20/11.12.2013)
12.
Bousselmi R, Lebbi MA, Ferjani M. Myocardial
Financial information and con ict of interest:
ischemic conditioning: Physiological aspects and clinical
e authors have no con ict of interest to declare.
applications in cardiac surgery. J Saudi Hear Assoc
2014; 26(2):93-100.
13.
Hausenloy DJ, Maddock HL, Baxter GF, Yellon DM.
References
Inhibiting mitochondrial permeability transition pore
opening: a new paradigm for myocardial preconditioning?
1. Murry CE, Jennings RB, Reimer KA. Preconditioning
Cardiovasc Res 2002;55(3):534-43.
with ischemia: a delay of lethal cell injury in ischemic
14.
Liu GS, Cohen M V, Mochly-Rosen D, Downey JM.
myocardium. Circulation 1986;74(5):1124-36.
Protein kinase C-epsilon is responsible for the protection
2. Marber MS, Latchman DS, Walker JM, Yellon DM.
of preconditioning in rabbit cardiomyocytes. J Mol Cell
Cardiac stress protein elevation
24 hours after brief
Cardiol 1999;31(10):1937-48.
16
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
15.
Costa ADT, Garlid KD, West IC, et al. Protein kinase
22.
Lu M, Atthe B, Mateescu G. Assessing mitochondrial
G transmits the cardioprotective signal from cytosol to
respiration in isolated hearts using 17O MRS. NMR
mitochondria. Circ Res 2005;97(4):329-36.
Biomed 2012;25(6):883-9.
16.
Gross GJ, Auchampach J A. Blockade of ATP-sensitive
23.
Perian M, Dobreanu D, Caldararu C, Sabau M. A
potassium channels prevents myocardial preconditioning
Simple ECG Recording Hardware for Langendor Isolated
in dogs. Circ Res 1992;70(2):223-33.
Heart Experiments. Fiziol - Physiol 2012;3(38):38-40.
17.
Pain T, Yang X-M, Critz SD, et al. Opening of
24.
E mov IR, Nikolski VP, Salama G. Optical Imaging of
Mitochondrial KATP Channels Triggers the
the Heart. Circ Res 2004;95(1):21-33.
Preconditioned State by Generating Free Radicals. Circ
25.
Yellon D, Alkhulai A, Pugsley W. Preconditioning the
Res 2000;87(6):460-6.
human myocardium. Lancet 1993;342(8866):276-7.
18.
Animal Care and Use Program. University of
26.
Noma A. ATP-regulated K+ channels in cardiac muscle.
California, Berkeley. Guidelines for Anaesthesia and
Nature 1983;305(5930):147-8.
Analgesia in Laboratory Animals. 2012;p 1-5.
27.
Cole WC, McPherson CD, Sontag D. ATP-regulated
19.
Arnaud C, Cracowski J-L, Hakim A, et al. 15-F2t-
K+ channels protect the myocardium against ischemia/
isoprostane and
5-F2t-isoprostane are not triggers of
reperfusion damage. Circ Res 1991;69(3):571-81.
myocardial preconditioning. Clin Exp Pharmacol
28.
Takagawa J, Zhang Y, Wong ML, et al. Myocardial
Physiol 2005;32(5-6):350-4.
infarct size measurement in the mouse chronic infarction
20.
Minasian SM, Galagudza MM, Dmitriev Y V,
model: comparison of area- and length-based approaches.
Kurapeev DI, Vlasov TD. Myocardial protection
J Appl Physiol 2007;102(6):2104-11.
against global ischemia with Krebs-Henseleit bu er-
29.
Nascimento DS, Valente M, Esteves T, et al. MIQuant-
based cardioplegic solution. J Cardiothorac Surg
semi-automation of infarct size assessment in models of
2013;8:60.
cardiac ischemic injury. PLoS One 2011;6(9):e25045.
21.
Gillis AM, Kulisz E, Mathison HJ. Cardiac
30.
Müllenheim J, Frässdorf J, Preckel B,
ämer V,
electrophysiological variables in blood-perfused and
Schlack W. Ketamine, but not S(+)-ketamine, blocks
bu er-perfused isolated, working rabbit heart. Am J
ischemic preconditioning in rabbit hearts in vivo.
Physiol Heart Circ Physiol 1996;271(2):H784-789.
Anesthesiology 2001;94(4):630-6.
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
17
Ex-Vivo Rat Hearts
Transmittal Letter
In consideration of the Medical Connections/Conexiuni Medicale taking action in reviewing and
editing the above-named Article, e ective upon acceptance of the Article by the Medical Connections/
Conexiuni Medicale (hereinafter re ered to as Med Con), the Autor(s) hereby assign(s) to the Med Con,
its legal representatives, successors and assigns, all publishing rights and each and every other right to the
Article throughout the world, in any language and in any medium, whether as an audiovizual work,
collective work, compilation, derivative work, joint work, literary work, phonorecord, pictorial, graphic or
sulptural work, sound recording, work of visual art, computer program, or any other medium now existing
or which hereafter may come into existence, including the copyright and the right to register the copyright
as well as the right to secure any renewals, reissues, and extensions of any such copyrights in Romania or
in any foreign country. Author(s) may request permission to reuse the manuscript or portions thereof.
Such requests must be in writing and permission by the Med Con shall not be unreasonably withheld. e
Author(s) appoint(s) the Med Con as the Author’s(s’) attorney-in-fact to execute any documents the Med
Con deems necessary to record any of these grants with the Romanian copyright o ce or elsewhere. e
Autor(s) also warrant(s) to the Med Con that the Article is original work of the Author(s) except for
material in the public domain and such excerpts from other works as may be included with the prior
written permission of the copyright owners; that the Article has not been previously published, submitted,
or accepted for publication elsewhere; that the Author(s) have no relationship, nancial or otherwise, with
any manufacturers or distributors of products evaluated in this paper, or alternatively any such relationship
has been disclosed in a footnote to the paper, or the requirement is irrelevant to this paper.
Manuscript Title: ___________________________________________________________
Name:
Signature/Date:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Please fax this signed form to the Med Con Editorial O ce.
Fax: +40-261-710456
ORIGINAL ARTICLES
HISTOPATHOLOGICAL COMPARATIVE ASSESSMENT OF
OSSEOINTEGRATION PROCESSES OF TITANIUM AND ZIRCONIUM
DENTAL IMPLANTS IN THE RABBIT FEMUR
Bogdan A Bumbu, Bogdan Uivărășeanu, Adrian G Bumbu, Traian T Maghiar
Faculty of Medicine and Pharmacy, University of Oradea
Address for correspondence:
Dr Bogdan Bumbu
Email: bogdanbumbu@yahoo.com
Received: 02.09.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 19-24
Abstract
Introduction
Titanium and zirconium implants were inserted
e use of biomaterials for implants into the hard
into the femur in 7 months rabbits bread under proper
tissues gains a larger acceptance in process of time. Since
and controlled conditions.
e rabbits were sacri ced
these are heterologous materials, it is of great importance
after three weeks, and
femurs harvested for
that before using any implant material, it should be
histopathological investigations.
e series
of
thoroughly studied for several issues. e implant needs
histopathological sections carried out through the bone
to show certain peculiar features for the organism to be
where the titanium implant has been integrated
tolerated, though it being perceived as an alien body.
permitted us to conduct assessments on the overall
Concurrently, the implant has to allow the proper
implanting area, from the connective tissue having
mending tissues proliferation in the vicinity till its full
covered the implant up to the medullary cavity. Provided
integration within the hard tissue
(bone).
e
we follow the consistency of the diaphysar bone we may
incorporation needs to be carried out adequately to
ascertain that it easily and progressively grows as we
secure the implant stability/resilience to mechanical
approach the implanting area and signi cantly grows in
applications (pressures, tensions etc.) that the relevant
its near vicinity.
e diaphysiary wall not only that it
area, subject to the integration, undergoes. For the
grew thicker outwards, but the outer third close to the
organism to tolerate it as much as possible and absorb it
implant shows an impacted bone on the most thorough
as consistently as possible within the hard tissue, the
zone of the entire diaphysiary wall and there are no
implant material must comprise a series of peculiar
periosteal bone proliferation processes to be identi ed
features.
ese features mainly refer to biocompatibility,
on the existing one for the titanium implant.
e
implant design and biomechanics [1].
osseointegration processes develop comparatively for
e biocompatibility refers to the relations and
both types of implants, but there is a mere di erence in
reactions establishing between the biomaterials and the
favor of the zirconium implant, where the bone
receiving tissues. In case of hard tissues, the
proliferation appears to be more advanced.
biocompatibility shows within the interface between the
Keywords: Osseointegration, Femur, Titanium,
implant and the bone proliferating in its vicinity. No
Zirconium
heterologous material will be completely tolerated by
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
19
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
the organism, since it is recognized by the immune
system as non-self. It is considered by the organism as an
intruder which however long it would persist in the
organism it will never be accepted as an inherent
structure. Nevertheless it is relevant the organism
reaction to an alien body and in terms of the material
qualities of which the implant is made of, the organism
may be more or less tolerating towards it. Whether the
tolerance is favorable, the organism will coat it all
around with its own tissue. Preserving the said form, it
can last within the organism for long period of time,
since the organism, though it will never consider it an
inherent structure, it will fail to naturally initiate
rejection reactions even consequently to its integration.
e implant design refers to its shape, size, with or
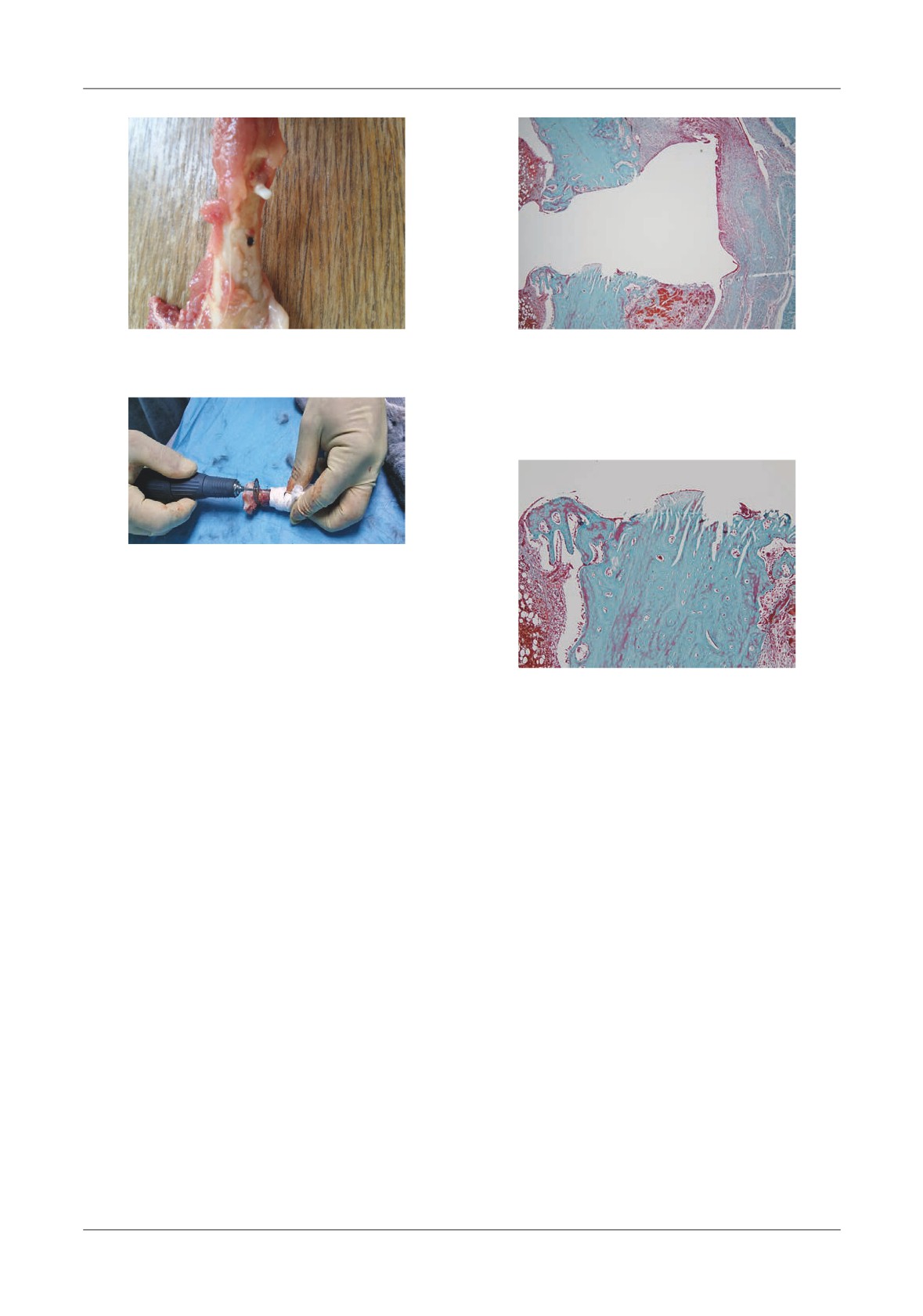
Figure 1. Preoperative care in sterile
conditions
without anchoring structures within the tissue (thread,
lead and height), but also to its mechanical features
(hardness and resistance).
e biomechanics refers to an implant mechanical
and dynamic feature in relation to the proximity tissues,
to how sustainable it is anchored within the organism
structures.
For studying the implants biocompatibility and
resistance, it proceeds to their integration into the cortical
or trabecular bone of testing animals in the femoral
condyle, the diaphysis of a long bone, cheek bone or
mandible [2]. For the outcome assessment secured during
the testing period it may be used the optical or electron
microscope, both showing advantages and limitations
[3].
e optical microscopy relies on the great advantage
of providing detailed information related to the entire
tissue area supporting the implant. e histopathological
Figure 2. e zirconium implant and the titanium
treatment of proliferated tissues in the vicinity of the
implant in the femur with primary stability
implant is though very laborious, so it is di cult to
process large series of samples. e laboratories equipped
with special section cutters able to bisect non-decalci ed
University of Medicine and Pharmacy Oradea biobase;
bones provide opportunities to secure information in
4 male rabbits of 3.5-4 kg and 40-50 cm and 4 female
shorter time, compared to the classical approach by
rabbits of 4-5 kg and 40-50 cm. e rabbits have been
decalci cation and para n treatment [4,5]. Considering
separated into 2 groups. For the rst group, titanium
the large amount of information provided by optical
implants (1AT) have been inserted, and titanium and
microscopy, it is still considered the ultimate method to
zirconium implants for the second batch.
e femur
assess the tissue response to an implant material [3].
implantation with titanium and/or zirconium implants
and consequently the rabbits killing have been carried
Material and Method
out in a surgery room completely observing the terms
and principles of a surgical procedure. e said operating
e studied material within this experiment on
room pertains to a private veterinary clinic, therefore we
rabbits is titanium and zirconium implants (taper shaped,
have bene ted from the professional support of a
lleted,
5 mm long) personalized ordered and
veterinarian colleague (Figure 1).
manufactured by S.C. Tehnomed Impex Co. SA Bucharest,
e implants were selected and sterilized properly.
a trading company specialized in medical materials.
e implants were implanted in surgery conditions in
Within the hereby study, we used 8 domestic rabbits
the rabbit femur, 1 cm from the joint.
e distance
of
7 months, common half-breed, issued from the
between the two implants was about 1,5 cm (Figure 2).
20
Bumbu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figure 3. Macroscopic appearance of the
Figure 5. Group 1AT - 3 weeks, the bone
femur taken for study
where the titanium implant has been
integrated. e diaphysiary bone easily and
progressively grows as approaching the
implanting area (Goldner’s Trichrome Method)
Figure 4. Sectioning the femur for histological
purpose
e experiment covered
4 months. Within the
hereby article, we will relate to the peri-implant
alterations occurred within the rst 3 weeks following
Figure 6. Group 1AT - 3 weeks, the bone
the implantation.
where the titanium implant has been
During the testing period, the rabbits have been
integrated. e necrotic bone resorption and
provided with proper conditions and constant
its partial replacement with a newly formed
monitoring: the temperature: 20-24ºC and day light
bone (Goldner’s Trichrome Method)
comprising a light-dark cycle of approximately 12/12
hours.
e animals have been fed during the entire
testing period with standard granulated feed and
overall implanting area, from the connective tissue having
discretionary fresh water.
covered the implant up to the medullary cavity (Figure 5).
At the end of the experimental period, the animals
Provided we follow the consistency of the
have been put to death and sampled the femur in order
diaphysiary bone we may ascertain that it easily and
to conduct histopathological studies (Figure 3).
progressively grows as we approach the implanting area
By means of a dental drill, the bone heads have been
and signi cantly grows in its near vicinity.
bisected to approximately
1 cm from the implant
e thickening of the diaphysiary bone within the
(Figure 4) and the pro led parts have been immediately
implant vicinity occurs both profoundly (it comes into
introduced into 10% formalin for xation.
prominence towards the medullary cavity) and super cially.
Following the decalci cation procedure, the parts
e bone aspect and structure within the implant vicinity
have been put into para n. Series of 5 µ sections have
are not identical on the entire surface, being identi ed
been carried out, colored through Goldner’s Trichrome
consistent di erences from one area to the other. erefore,
Method.
the middle area shows a structural modi ed bone
consequently the traumatism while conducting the
Results
experimental fault required for the implant integration.
e said traumatism engendered a bone necrotic zone
e series of histopathological sections carried out
in ltrating to a certain depth into the bone wall.
through the bone where the titanium implant has been
ough we may notice a certain mending activity
integrated permitted us to conduct assessments on the
advancing from the bone depth towards the contact
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
21
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
surface with the implant, the necrotic bone resorption and
e overall picture provides information related to
its replacement with a newly formed bone only partially
the zirconium implant zone and its e ects on the hard
succeeded till this point into the experiment, showing
and soft structures to an extent allowing the assessment of
di erences from one zone to the other (Figure 6).
the surgery traumatism e ects and the recovery processes
It is a whole di erent situation for the super cial
up to a long distance from the implant (Figure 9).
and profound zones of the diaphysiary bone within the
e aspects of most interest are to be found on the
implant vicinity, where the bone is in proliferation and
interface bone
- implant and they can be correctly
expansion process, so that the contact surface with the
assessed on the histopathological section. One can
implant is obviously wider than the diaphysiary bone
determine that the bone wall follows intimately the
initial thickness.
e bone on the surface of the
implant super cies and up to the medullary canal.
experimental fault looks necrotic only on a thin zone
As for overall surface, the osseointegration appears
(the zone intimately touching the implant), and
to be in a more advanced phase than in the case of the
otherwise it shows a trabecular bone aspect with obvious
titanium implant, the impacted bone zone to be
proliferation and expansion predisposition.
erefore,
progressively eliminated appears here clearly thinner
coming out of the implant, the bone on the diaphysis
(Figure 10).
surface shows sporadically areoles and proliferation
Also, for the zirconium implant, the diaphysiary
predisposition towards periosteum, either through the
wall within the close vicinity of the implant thickened,
formation of new trabeculae or the proliferation of
but not in both directions, as for the titanium implant.
subperiosteal bone with primary bone aspect, where one
e diaphysiary wall not only that it grew thicker
can identify a certain predisposition for forming areoles.
outwards, but the outer third close to the implant shows
e existing areoles in all these zones include a large
an impacted bone on the most thorough zone of the
number of osteoblasts (Figure 7) suggesting an intense
entire diaphysiary wall and there are no periosteal bone
bone proliferation.
proliferation processes to be identi ed on the existing
is recent bone structuring progressively within
one for the titanium implant. A discrete predisposition
the subperiosteal zone will constitute a resistance
of bone proliferation within the subperiosteal zone is
structure required to enhance the implant zone that has
identi ed only to a given distance from the implant
mechanically weakened consequently to the
zone.
experimental bone fault carrying out.
We have a whole di erent situation for the central
Together with the bone proliferation processes there
third and mainly the inner implant zone where the bone
are bone resorption processes needed to remove all bone
tissue reconstruction may be assessed as very consistent
structures a ected following the surgery trauma.
e
considering three weeks have passed since the operation.
existence of bone resorption is shown by the existence of
Here there is only a thin layer of impacted bone, in close
osteoclasts intimately touching the impacted bone
contact with the implant, but analyzing the aspect, it
(Figure 8).
will be resorbed in a relatively short matter of time and
e profound zone of the bone wall within the
replaced by a newly formed bone. e diaphysiary bone
implant vicinity is made of trabecular bone signi cantly
in the implant zone extends towards the internal
exceeding the inner edge of the diaphysiary bone. It is
diaphysiary cavity by a boned extension closely following
newly formed areolar bone where one can still identify
the implant, and as for its structure it is an areolar bone
rare bone fragments with vestigial aspect derived from
with peculiar aspect of recent bone [6].
e areoles of
the traumatism caused by the experimental bone fault
this bone include multiple osteoblasts establishing it is
carrying out.
e trabeculae of the areolar bone
subject to a proliferation process (Figure 11).
comprise on their environs an impressive number of
In the diaphysiary bone internal part it is ascertained
osteoblasts, showing that the bone proliferation activity
for this implant as well the bony wall thickening by the
is under way. e said trabecular bone continues on the
proliferation of a bony sleeve that can be traced
diaphysis side of the medullary canal by a segment of
throughout a relatively long distance and that thins
partially areolar bone whose thickness decrease while
while receding from the implant zone. Here as well it
receding from the implant zone. It is still a resistance
represents
an internal
compacting structure
structure compacting from the inside the bone
compensating the momentarily mechanical resistance
surrounding the implant. ere are multiple osteoblasts
weakening of the implant zone.
both within the areoles of this bone sleeve and on its
Concurrently with these bone proliferation active
surface, suggesting that these compacting structures will
processes, we identi ed aspects related to bony structures
continue to extend.
lyses required to eliminate the compromised bony
22
Bumbu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figure 7. Group 1AT - 3 weeks, the bone
Figure 10. Group 1AZ - 3 weeks, the bone
where the titanium implant has been
where the zirconium implant has been
integrated. e density of the proliferation of
integrated. e comparative evolution of
osteoblasts in the bone (Goldner’s Trichrome
osseointegration for the two types of implant
Method)
(Goldner’s Trichrome Method)
Figure 8. Group 1AT - 3 weeks, the bone
Figure 11. Group 1AZ - 3 weeks, the bone
where the titanium implant has been
where the zirconium implant has been
integrated. e presence of osteoclasts in
integrated. e process of bone proliferation
intimate contact with the bone a ected
evidenced by the presence of high number of
(Goldner’s Trichrome Method)
osteoblasts (Goldner’s Trichrome Method)
Figure 9. Group 1AZ - 3 weeks, the bone where
Figure 12. Group 1AZ - 3 weeks, the bone
the zirconium implant has been integrated.
where the zirconium implant has been
E ects of operator trauma and rehabilitation
integrated. Osteoclasts at the level of presence
processes in relation to the distance to the
to experimental bone defect (Goldner’s
implant (Goldner’s Trichrome Method)
Trichrome Method)
compounds while carrying out the experimental fault
zone and at a given distance from it. In the areas where
and impacted by the in ammatory and post-surgery
bone fragments detached while carrying out the
necrotic processes.
eir existence is pictured by the
experimental bone fault lasted, the number of osteoclasts
presence of osteoclasts both within the implant contact
is very consistent (Figure12).
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
23
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Discussions
Conclusions
Looking at the bone tissue surrounding the two types
ree weeks after the integration of the two types of
of implant, we may ascertain that they are in close contact
implants, the osseointegration processes are consistently
with the implant material, attending all its accidents. No
progressing and with a markedly intensity, the newly
rejection reaction from the organism has been noticed in
formed bone already coating the implants on a given
either case of the studied implants. e injuries following
surface and presents a distinct predisposition to extend
the experimental fault carrying out while the implant was
on end.
e osseointegration processes develop
integrated disappeared for the most part through the
comparatively for both types of implants, but there is a
proliferation of recent boned structures penetrating from
mere di erence in favor of the zirconium implant,
the bone deepness towards the contact surface with the
where the bone proliferation appears to be more
implant. For the most part of contact surface with the
advanced.
implant, the bone is reconstructed, though it appears as a
recent bone undergoing progressive remolding and
compacting processes.
e reconstruction processes
References
evolved so well that the newly formed bone extends over
the implant accidents for a given distance, making the
1.
Osborn JF, Newesley H. Dynamics aspects of the bone-
bone-implant surface to be thicker than the diaphysiary
implant interface. In Heimke G, ed: Dental implants-
bone surface where the bone fault has been carried out.
material and systems. Hanser, Munich, 1980;pp 111-
is extension of the newly formed bone occurs primarily
23.
within the internal part of the experimental fault and
2.
Tencer AF. Osteocompatibility. In von Recum AF, ed:
leaves the impression that it will continue coating the
Handbook of Biomaterials Evaluation. Taylor and
implant with bony structures on a surface growingly larger.
Francis, Philadelphia, PA, 1999:539-66.
Furthermore, the newly formed bone extends to the
3.
John A. Jansen. Histological Analysis of Bone-Implant
internal part of the diaphysiary bone to a certain extent,
Interface. From: Handbook of Histology Methods for
getting to the zonal thickening and the increasing
Bone and Cartilage, Edited by: Y. H. An and K. L.
resistance of the diaphysiary bone surrounding the
Martin, Humana Press Inc., Totowa, NJ, 2003, 353-
implants. ese aspects show a consistent evolution of the
60.
osseointegration processes, though they require a long
4.
Donath K, Breuner G. A method for the study of
period of time in order to conclude. e three weeks only
undecalci ed bones and teethwith attached soft tissues.
since the integration of the implants are not su cient to
e Säge-Schli
(sawing and grinding) technique. J
achieve the osseointegration processes.
e aspect is
Oral Pathol 1982;11(4):318-26.
pictured by the fact that on the bone-implant interface we
5.
van der Lubbe HB, Klein CP, de Groot K. A simple
may mark out the degenerated acellular bone, but only for
method for preparing thin
(10microM) histological
circumscribed areas which are to be found within the
sections of undecalci ed plastic embedded bone with
external half of the diaphysiary bone exclusively.
e
implants. Stain Technol 1988;63(3):171-6.
thickness of the said degenerated bone is slightly di erent
6.
Erlandsen S L, Magney J E. Color Atlas of Histology,
from one zone to the other, but for the overall bone -
Mosby Year Book, St. Louis, 1992
implant surface the di erences are not signi cant between
7.
Black J. Biological Performance of Materials. Marcel
the two types of implants. Nevertheless, at this point of the
Dekker Inc., New York, NY, 1992.
experiment it appears that the osseointegration processes
8.
Carl Hanser Verlag. Dental Implants: Materials and
are sensibly more advanced for the zirconium implant.
Systems. Munich, Germany, 1980:111-23.
24
Bumbu et al
ORIGINAL ARTICLES
A COMPARATIVE CASE STUDY OF ACUTE ABDOMEN IN DIABETIC
AND NON DIABETIC PATIENTS
Dănu Dejeu1,2, Aurel Babeș2
1Surgery I Clinic, County Clinic and Emergency Hospital, Oradea, 2Facultaty of Medicine and Pharmacy, University of
Oradea
Address for correspondence:
Dr. Dănu Dejeu
Str. Gh. Doja nr. 184 A, Oradea
E-mail: dandejeu@yahoo.com
Received: 01.09.2014
Accepted: 30.09.2014
Med Con October 2014, Vol 9, No 3, 25-34
Motto: “It is better to have regrets in surgery than face consequences at autopsy” - I. IACOBOVICI
Abstract
diabetics (9.84% vs. 5.38%). e average duration of
hospitalization in the Surgery I clinic was 3.8 days, 5.1
Introduction: We proposed to analyze the impact
days for acute abdomen cases, while in diabetic patients
of hyperglycemia on the evolution of acute abdomen in
with acute abdomen the average duration of
comparison to non-diabetic patients, on morbidity and
hospitalization is 7.8 days.
mortality rates, duration of hospitalization.
Conclusion: e study demonstrates a di erence in
Method:
is observational, retrospective and
patient’s evolution, complications, mortality as well as
group study was conducted in the period 2008-2011,
the duration of hospitalization in diabetic versus non
on 4,021 cases of acute abdomen admitted in the
diabetic patients.
Surgery I clinic of the Emergency Hospital, Oradea. Of
Keywords: acute abdomen, diabetics, non-
these 488 were diabetic patients and 3,533 nondiabetic
diabetics, morbidity, mortality
patients.
Result: Females predominated in both groups
Introduction
(62.24% versus
58.40%). Majority of the patients
(62.37%) with an acute abdomen were between the ages
Acute abdomen can be de ned as an intra-
of 30-69 years, with a signi cant statistical di erence
abdominal pathological process which generally causes
(p<0.0001). Vascular forms, acute pancreatitis and false
intense pain and requires an immediate decision, in the
acute abdomen were signi cantly more frequent in
majority of cases a surgical intervention is considered
diabetic patients in comparison to the non-diabetic.
[1,2]. General causes of acute abdomen are:
Peritonitic form was more frequent in the non-diabetic,
in ammation, mechanical, vascular, trauma and acute
with a signi cant statistical di erence
(p=0.0003).
pancreatitis [3]. In ammatory causes can be divided into
Postoperative morbidity of 36.27% was seen in diabetic
two categories: bacterial
(acute appendicitis, acute
patients, presenting a signi cant percentage higher than
diverticulitis, and acute cholecystitis) and chemical
that of non-diabetic patients (14.43%). Mortality in
(perforated gastro-duodenal ulcer).
e mechanical
diabetic patients was signi cantly higher than in non-
category refers to incarcerate hernias, post-operatory
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
25
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table I. Distribution of cases according to sex
Year 2008
Year 2009
Year 2010
Year 2011
Total
Sex
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Non-diabetic
Females
460
61.17
493
63.53
502
62.67
744
61.79
2,199
62.24
Males
292
38.83
283
36.47
299
37.33
460
38.21
1,334
37.76
752
776
801
1,204
3,533
p†
p<0.0001*
Diabetic
Females
67
58.26
64
57.66
60
57.69
94
59.49
285
58.40
Males
48
41.74
47
42.34
44
42.31
64
40.51
203
41.60
115
111
104
158
488
p†
p=0.0004*
Total
Females
527
60.78
557
62.80
562
62.10
838
61.53
2,484
61.78
Males
340
39.22
330
37.20
343
37.90
524
38.47
1537
38.22
867
887
905
1,362
4,021
p†
p<0.0001*
p<0.05 shows a statistically signi cant di erence between the groups studied
*Comparison of proportions test
adherence, torsions, and neoplastic obstructions of the
diabetic patients and 3,533 non-diabetic patients. is
colon.
e vascular category produce acute abdomen
study was approved by the internal advisory committee
through mesenteric thrombosis or embolism followed
of research and development of the hospital.
by intestinal necrosis and gangrene. Traumatic causes
e statistical analysis methods used were the Chi-
refer to open abdominal wounds, abdominal trauma
squared test, Fisher’s exact test, Comparison of means
with spleen or liver rupture [4].
test, Comparison of proportions test, Relative risk test
It is essential to recognize when an acute abdomen
and the calculation of correlation coe cient using the
emergency exists, for which an immediate surgical
statistical medical program MedCalc® version 12.2.1.0
intervention is required and should not be delayed [5].
(MedCalc® Software, Mariakerke, Belgium).
Patients present with diverse symptoms ranging from
pain, collapse, shock, but not all these clinical
Results
characteristics are present in every patient [6]. Severe
pain is the most frequent symptom and is often
Patients
generalized [7]. e essential dilemma arises in a diabetic
Females predominated in the study (61.78% vs.
patient with ketoacidosis and signs of acute abdomen.
38.22%), resulting in a female/male ratio of 1.6:1. In
e installation of ketoacidosis can be a consequence of
the non-diabetics, the female/male ratio was 1.6, while
a nonsurgical conditions, and digestive signs due to
the diabetics had a ratio of 1.4 (Table I).
metabolic decompensation or may be secondary to true
Analyzing case distribution according to age, the
acute abdomen [8]. We aim to determine the impact of
majority of patients (62.37%) with acute abdomen were
peri, intra and post-operative hyperglycemic phases, on
between the ages of 30-69 years, with a signi cant
the evolution of diabetic and non diabetic patients with
statistical di erence (p<0.0001) (Table II).
acute abdomen, namely, on the morbidity and mortality
e average age in the diabetics was signi cantly
rates, duration of hospitalization, etc.
higher than that of non-diabetics (62.14 years vs. 49.37
years) (p<0.0001) (Table II).
Material and Method
In the group of non-diabetic patients with acute
abdomen, over 60% were between the ages of 30-69
is observational, retrospective and group study
years, with a signi cant statistical di erence
was conducted in the period 2008-2011, on 4,021 cases
(p<0.0001),while in the group of diabetic patients with
of acute abdomen admitted in the Surgery I Clinic of
acute abdomen, majority (85.86%) was above 50 years
the Emergency Hospital, Oradea.
ere were
488
of age (p<0.0001) (Table II).
26
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Table II. Case distribution according to age
Age/
Year 2008
Year 2009
Year 2010
Year 2011
Total
years
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Non-diabetic
<30
168
22.34
161
20.75
180
22.47
249
20,68
758
21.45
30-49
196
26.06
209
26.93
219
27.34
295
24,50
919
26.01
50-69
262
34.84
272
35.05
273
34.08
439
36.46
1,246
35.27
≥70
126
16.76
134
17.27
129
16.10
221
18.36
610
17.27
p†
p<0.0001*
A***.mean
48.83±5.52
49.06±6.01
48.46±5.78
50.25±5.87
49.37±5.72
Diabetic
<30 years
3
2.61
2
1.80
2
1.92
6
3.80
13
2.66
30-49
11
9.57
13
11.71
15
14.42
17
10.76
56
11.48
50-69
68
59.13
68
61.26
60
57.69
91
57.59
287
58.81
≥70
33
28.70
28
25.23
27
25.96
44
27.85
132
27.05
p†
p<0.0001*
A. mean
62.81±7.21
62.34±6.97
61.59±7.14
61.87±7.26
62.14±6.92
p†
Non-diabetic
49.37±5.72
Diabetic
62.14±6.92
p<0.0001**
Total
<30
171
19.72
163
18.38
182
20.11
255
18.72
771
19.17
30-49
207
23.88
222
25.03
234
25.86
312
22.91
975
24.25
50-69
330
38.06
340
38.33
333
36.80
530
38.91
1,533
38.12
≥70
159
18.34
162
18.26
156
17.24
265
19.46
742
18.45
p†
p<0.0001*
A. mean
50.69±6.45
51.06±6.24
49.97±6.05
51.60±5.75
50.92±6.15
†p<0.05 shows a statistically signi cant di
erence between the groups studied
* Chi-square test
** Comparison of means test
A*** Average mean
Diabetes mellitus type 1 was only seeing in 4.10%
Table III. Characteristics of diabetic patients
of diabetic patients, the majority had Diabetes mellitus
with acute abdomen
type 2 (95.90%) (p<0.0001) (Table III).
Majority of the cases had a duration of evolution of
Type of Diabetes mellitus Nr.
%
p†
diabetes over 10 years (34.43%). We noted an important
DM type 1
20
4.10
proportion of patients diagnosed with diabetes mellitus
p<0.0001*
DM type 2
468
95.90
on admission (16.39%) (Table III).
Duration of diabetic mellitus
Majority of the diabetic patients had therapy with
Diagnosis on admission
80
16.39
oral anti-diabetic drugs (57.79%). 25.82% were Insulin
<1 year
61
12.50
dependent, of which 15.16% had mixed therapy (OAD
1-5 year
100
20.49
p<0.0001*
+ insulin).
e percentage of those without therapy
5-10 year
79
16.19
(16.39%) represents the cases of diabetes detected on
admission (Table III).
>10 year
168
34.43
An analysis of the average duration of onset of acute
Anti-diabetic therapy
abdomen on admission , revealed an average of 33.52
Without therapy
80
16,39
hours before admission, with a signi cantly higher
OAD
282
57.79
p<0.0001*
duration in males compared to females (35.64 hours vs.
Insulin
52
10.66
29.04 hours) (p<0.0001) (Table IV). In the non-diabetic,
OAD + insulin
74
15.16
the duration of onset on admission was signi cantly
†p<0.05 shows a statistically signi cant di erence between the
higher in males than in female (34.56 hours vs. 29.04
groups studied
hours) (p<0.0001), while in the diabetic, the duration was
* Chi-square test
signi cantly higher in females than in males (56.64 hours
OAD - oral anti-diabetics
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
27
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table no. IV. Duration of onset on admission (hours) of acute abdomen).
Patients
Females
Males
p†
Total
p†
Non-diabetic
29.04±3.75
34.56±4.50
p<0.0001*
31.20±4.27
p<0.0001*
Diabetic
56.64±6.86
42.72±5.32
p<0.0001*
50.85±6.28
Total
32.21±4.87
35.64±4.72
p<0.0001*
33.52±4.92
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of means test
Table V. Average glycemic level in patients studied
Mean average of glycemia
Total patients Non-diabetic
Diabetic
p†
(mg/dL)
(n=4021)
(n=3533)
(n=488)
Before surgical intervention
120.4±37.9
112.6±28.2
154.42±17.82
p<0.0001*
Day of surgical intervention
137.6±33
132.2±27.6
160.89±19.44
p<0.0001*
After surgical intervention
119.9±26.5
114.5±21.2
147.91±19.20
p<0.0001*
†p<0.05 shows a statistically signi cant di erence between the groups studied
*Comparison of means test
Table nr. VI. Distribution of cases according to the clinical form of acute abdomen
Nondiabetic
Diabetic
Total
Form
p†
Nr.
% Nr.
% Nr.
%
Peritonitic
2,158
61.08
256
52.46
2,414
60.03
p=0.0003*
Occlusive
894
25.30
121
24.80
1,015
25.24
p=0.8516*
Hemorrhagic
142
4.02
22
4.51
164
4.08
p=0.6967*
Organ torsion
28
0.79
7
1.43
35
0.87
p=0.2416*
Vascular
34
0.96
20
4.10
54
1.34
p<0.0001*
Acute pancreatitis
256
7.25
52
10.66
308
7.66
p=0.0103*
False acute abdomen
21
0.59
10
2.05
31
0.77
p=0.0015*
Total
3,533
488
4,021
†p<shows a statistically signi cant di erence between the groups studied
* Chi-square test
versus 42.72 hours) (p<0.0001). e duration of onset of
Clinical hyperglycemia (de ned as a blood glucose
abdominal diseases on admission was signi cantly higher
level >180 mg/dL) was observed in 7.78% (38) of the
in diabetic patients in comparison to the non-diabetic
diabetic patients before the surgical intervention, in
(50.85 hours vs. 31.20 hours) (p<0.001) (Table IV).
17.2% (84) of diabetic patients on the day of surgery
e blood glucose level before the surgical
and 9.83% (48) of diabetic patients in the postoperative
intervention in the study group was 120.4±37.9 mg/dL.
period (2-10 days).
As was anticipated, the non-diabetic patients had lower
Clinical Forms
peri-operatory glycemic levels (112.6±28.2 mg/dL) in
e most frequent cause of acute abdomen was
comparison to patients with a history of diabetes
peritonitis
(60.3%), followed by occlusion
(25.4%),
(154.42±17.83 mg/dL, p<0.0001). e blood glucose
acute pancreatitis (7.66%) hemorrhagic form (4.08%)
level in the rst day after surgery was 160.89±19.44 mg/
and other causes (less than 1.5%) (Table VI).
dL in patients with diabetes mellitus and 132.2±27,6
Peritonitic acute abdomen
mg/dL in non-diabetic patients; both values were higher
e most frequent cause of peritonitis in the whole
than those reported in the subsequent period of
study group
(diabetic+non-diabetic) was acute
hospitalization (147.91±19.20 and 114.5±21.2 mg/dL,
appendicitis
(24.73%), acute cholecystitis
(22.12%),
respective, p<0.0001) (Table V).
small and large intestinal perforations (17.94%) and
After surgery, 3.99% (192) of the diabetic patients
perforated gastro-duodenal ulcer (12.92%), followed by
had a glycemic level >140 mg/dL; three quarters of these
acute diverticulitis
(8.53%) and postoperative
(144) had a glycemic level between 141 and 180 mg/dL,
complications (7.37%), the remaining causes having a
while the rest (48) had a glycemic level >180 mg/dL.
percentage less than 3% (Table VII)
28
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Table VII. Distribution of patients with peritonitic acute abdomen according to determining lesion
Nondiabetic
Diabetic
Total
Cause
p†
Nr.
%
Nr.
%
Nr.
%
Acute appendicitis
544
25.21
53
20.70
p=0.5761*
597
24.73
Acute cholecystitis
486
22.52
48
18.75
p=0.6762*
534
22.12
Acute diverticulitis
178
8.25
28
10.94
p=0.9130*
206
8.53
Perforated gastro-duodenal ulcer
286
13.25
26
10.16
p=0.8855*
312
12.92
Small and large intestinal perforations
391
18.12
42
16.41
p=0.9499*
433
17.94
Biliary peritonitis
40
1.85
12
4.69
p=0.6164*
52
2.15
Gynecological diseases- peritonitis
41
1.90
8
3.13
p=0.2603*
49
2.03
Peritoneal dialysis
6
0.28
2
0.78
p<0.0001*
8
0.33
Hepatic/splenic abscess
7
0.32
3
1.17
p<0.0001*
10
0.41
Postoperative
153
7.09
25
9.77
p=0.9503*
178
7.37
Ruptured perinephric peritoneal collections
2
0.09
2
0.78
p<0.0001*
4
0.17
Primitive peritonitis
5
0.23
2
0.78
p<0.0001*
7
0.29
Others
19
0.88
5
1.95
p=0.0276*
24
0.99
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
Table VIII. Germs implicated in peritonitic acute abdomen
Non-diabetic
Diabetic
Total
Cause
p†
Nr.
%
Nr.
%
Nr.
%
E.coli
1.467
67.98
143
55.86
p=0.0044*
1.610
66.69
Pseudomonas
486
22.52
48
18.75
p=0.6762*
534
22.12
Proteus
178
8.25
28
10.94
p=0.9130*
206
8.53
Serratia
286
13.25
26
10.16
p=0.8855*
312
12.92
Candida
391
18.12
42
16.41
p=0.9499*
433
17.94
Aerobacter
40
1.85
12
4.69
p=0.6164*
52
2.15
Klebsiella
41
1.90
8
3.13
p=0.2603*
49
2.03
Anaerobes
6
0.28
2
0.78
p<0.0001*
8
0.33
Bacteroides
7
0.32
3
1.17
p<0.0001*
10
0.41
Streptococci
153
7.09
25
9.77
p=0.9503*
178
7.37
Staphylococci anaerobes
2
0.09
2
0.78
p<0.0001*
4
0.17
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
From the point of view of determining lesions
Occlusive acute abdomen
signi cant di erences exists between the diabetic and non-
In the diabetic, as well the non-diabetic, the most
diabetic in the cases of peritoneal dialysis, hepatic/splenic
frequent primary lesions in occlusive acute abdomen,
abscesses and ruptured perinephric peritoneal collections,
were eventrations and hernias (40.50% vs. 39.37%),
primitive peritonitis and other causes (p<0.05).
followed by parietal causes
(tumors, in ammations,
Analyzing the frequency of germs involved in acute
stenosis) (29.75 vs. 31.54%) and extra-parietal causes
abdomen peritonitis , we found that E. coli was the
(23.14% vs. 20.13%), there are no signi cant di erences
germ involved in most cases (66.69%) , both in the
between the study groups (p>0.05). e average duration
diabetic and non-diabetic with a statistically signi cant
of hospitalization for occlusive acute abdomen was 5.29
di erence between the two groups in comparison with
days, signi cantly higher in the diabetic compared to the
other germs (p=0.0044) (Table VIII).
non-diabetic (6.80 vs. 5.11 days) (p<0.0001) (Table IX)
e average duration of hospitalization of acute
Hemorrhagic acute abdomen
abdomen caused by peritonitis was
5.29 days,
Majority of the cases of hemorrhagic acute abdomen
signi cantly higher in the diabetic compared to the
were caused by trauma (68.29%), ruptured ovarian cyst
non-diabetic (6.80 vs. 5.11 days) (p<0.0001)
and extra-uterine pregnancy made up
18.29% and
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
29
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table IX. Distribution of patients with occlusive acute abdomen according to the primary lesion
and the average duration of hospitalization (ADH)
Nondiabetic
Diabetic
Total
p†
Nr.
%
Nr.
%
Nr.
%
Extraparietal (compressive abdominal
180
20.13
28
23.14
p=0.9082*
208
20.49
tumors, obstructions, adherences)
Parietal (tumors, in ammations, stenosis)
282
31.54
36
29,75
p=0.9783*
318
31.33
Intraluminal (fecaloma, biliary stones,
32
3.58
4
3.31
p=0.1599*
36
3.55
foreign bodies)
Eventrations, hernias
352
39.37
49
40.50
p=0.9965*
401
39.51
Secondary dynamic ileus
48
5.37
4
3.31
p=0.3209*
52
5.12
p†
p<0.0001**
Total
894
121
1.015
DMS
5.11±0.60
6.80±0.72
p<0.0001***
5.29±0.66
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
** Chi-square test
*** Comparison of means test
Table X. Distribution of patients with hemorrhagic acute abdomen according to the primary lesion
Non-diabetic
Diabetic
Total
p†
Nr.
%
Nr.
%
Nr.
%
Trauma
95
66.90
17
77.27
p=0.5727*
112
68.29
• splenic
42
29.58
8
36.36
p=0.9704*
50
30.49
• hepatic
17
11.97
3
13.64
p=0.4059*
20
12.20
• mesenteric
12
8.45
3
13.64
p=0.4082*
15
9.15
• associative
24
16.90
3
13.64
p=0.4960*
27
16.46
Extra-uterine pregnancy
17
11.97
2
9.09
p=0.2963*
19
11.59
Ruptured ovarian cyst
28
19.72
2
9.09
p=0.5738*
30
18.29
Others
2
1.41
1
4.55
p=0.0002*
3
1.83
p†
p<0.0001**
Total
142
22
164
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
** Chi-square test
11.59% respectively, with a signi cant statistical
statistical di erence,
(Table XII).
e most frequent
di erence (p<0.0001) (Table X).
interventions were annexectomies (46.88%), followed
Of the 164 cases of hemorrhagic acute abdomen,,
by sigmoid resections
(34.38%), with a signi cant
128 cases (78.05%) had undergone surgical intervention,
statistical di erence
(p=0.0573). No signi cant
a non-signi cant di erence in the non-diabetic in
di erence existed between the diabetic and non-diabetic
comparison to the diabetic (p=0.8172) (Table XI). Most
regarding the type of surgical intervention (p>0.05).
of these patients had undergone splenectomy (39.06%),
Vascular acute abdomen (enteromesenteric infarct)
followed by annexectomies and salpingectomies,
Vascular acute abdomen occurred more frequently
(17.97% and 14.84% respectively), with a signi cant
in the diabetic than the non-diabetic (4.10% vs. 0.96%,
statistical
di erence
(p<0.0001)
(Table XI).
p<0.0001). Majority of the cases had mesenteric infarct
Enterectomies and omentum hemostasis were more
of a segment of the small intestine (37.04%), followed
frequent in diabetic patients
(5.88% vs.
4.50%,
by all of the small intestine and large intestine, each
p=0.0117, 5.88% vs. 1.80%, p=0.0009 respectively).
making up 22.22% of the cases. 18.52% of the cases
Organ torsion
represented localization only at the level of the large
Majority of organ torsions were female genital tubes
intestine (Table XIII).
(42.86%), followed by sigmoid volvulus (37.14%) and
All cases of vascular acute abdomen had undergone
volvulus of the small intestine without a signi cant surgical intervention. Exploratory laparotomy was carried
30
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Table XI. Surgical interventions carried out for hemorrhagic acute abdomen
Non-diabetic
Diabetic
Total
p†
Nr.
%
Nr.
%
Nr.
%
Splenectomy
42
37.84
8
47.06
p=0.9248*
50
39.06
Hepatorrhaphy
15
13.51
3
17.65
p=0.4725*
18
14.06
Atypical hepatic resection
2
1.80
-
-
2
1.56
Enterectomies
5
4.50
1
5.88
p=0.0117*
6
4.69
Omental hemostasis
2
1.80
1
5.88
p=0.0009*
3
2.34
Salpingectomies
17
15.32
2
11.76
p=0.3603*
19
14.84
Annexectomies
21
18.92
2
11.76
p=0.4797*
23
17.97
Ovarian chistectomy
7
6.31
-
-
7
5.47
p†
p<0.0001**
Total
111
78.17
17
77.27
p=0.8172*
128
78.05
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
** Chi-square test
Table XII. Distribution of patients according to the cause of organ torsion
Non-diabetic
Diabetic
Total
p†
Nr.
%
Nr.
%
Nr.
%
Sigmoid volvulus
11
39.29
2
28.57
p=0.6132*
13
37.14
Adnexal torsion (tumor, cyst)
12
42.86
3
42.86
p=0.5143*
15
42.86
Small intestine volvulus
5
17.86
2
28.57
p=0.4754*
7
20.00
p†
p=0.1077**
Total
28
7
35
Surgical interventions in acute abdomen caused by organ torsion
Enterectomies
4
16.00
2
28.57
p=0.4733*
6
18.75
Annexectomies
12
48.00
3
42.86
p=0.6262*
15
46.88
Sigmoid resections
9
36.00
2
28.57
p=0.5342*
11
34.38
p†
p=0.0573**
Total
25
89.29
7
100
p=0.8172*
32
91.43
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Comparison of proportions test
** Chi-square test
Table XIII. Patient distribution according to the extent of entero-mesenteric infarct
Non-diabetic
Diabetic
Total
p†
Nr.
%
Nr.
%
Nr.
%
Total small intestine
10
29.41
2
10.00
p=0.174083*
12
22.22
Small intestine segment
8
23.53
12
60.00
p=0.010013*
20
37.04
Large intestine
6
17.65
4
20.00
p=1.000000*
10
18.52
Small + large intestine
10
29.41
2
10.00
p=0.174083*
12
22.22
p†
p=0.1203**
Total
34
0.96%
20
4.1%
54
Surgical intervention in acute abdomen caused by entero-mesenteric infarct
Enterectomies
8
23.53
12
60.00
p=0.010013* 20
37.04
Colectomy
6
17.65
4
20.00
p=1.000000*
10
18.52
Exploratory laparotomy
20
58.82
4
20.00
p=0.009911* 24
44.44
p†
p=0.0131**
Total
34
100
20
100
54
100
†p<0.05 shows a statistically signi cant di erence between the groups studied
* Fisher’s exact test
** Chi-square test
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
31
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table XIV. Patient distribution according to causes and morphological forms of acute pancreatitis
Non-diabetic
Diabetic
Total
Cause
p†
Nr.
% Nr.
%
Nr.
%
Biliary
144
56.25
30
57.69
p=0.879197*
174
56.49
Toxic
56
21.88
7
13.46
p=0.191674*
63
20.45
Dysmetabolic
38
14.84
12
23.08
p=0.151117*
50
16.23
Others
18
7.03
3
5.77
p=1.000000*
21
6.82
p†
p<0.0001**
Total
256
7.25
52
10,66
308
Morphopathologic forms
Edematous
112
43.75
15
28.85
p=0.062976*
127
41.23
Necrotic-hemorrhagic
99
38.67
24
46.15
p=0.352595*
123
39.94
Pancreatic abscess
45
17.58
13
25.00
p=0.242703*
58
18.83
p†
p<0.0001**
Total
256
52
308
†p < 0,05 shows a statistically signi cant di erence between the groups studied
* Fisher’s exact test
** Chi-square test
Table XV. Patient distribution according to the type of emergency in acute pancreatitis
Non-diabetic
Diabetic
Total
Type of emergency
p†
Nr.
% Nr.
%
Nr.
%
Immediate emergency
20
7.81
15
28.85
p=0.000543*
35
11.36
Delayed emergency
42
16.41
8
15.38
p=0.537962*
50
16.23
Late emergency
91
35.55
14
26.92
p=0.026192*
105
34.09
p†
p<0.0001**
Total
153
59.77
37
71.15
190
61.69
Type of emergency operated
Immediate emergency
20
13.07
14
43.75
p=0.000195*
34
18.38
Delayed emergency
42
27.45
6
18.75
p=0.379246*
48
25.95
Late emergency
91
59.48
12
37.50
p=0.030772*
103
55.68
p†
p<0.0001**
Total
153
100
32
100
185
100
Surgical intervention in acute abdomen for pancreatitis
Cholecystectomy - laparotomy
42
27.45
11
34.38
p=0,847992*
53
28.65
Cholecystectomy - laparoscopy
82
53.59
12
37.50
p=0.001230*
94
50.81
Cholecystectomy + EBD
18
11.76
7
21.88
p=0,293086*
25
13.51
Necresectomy
40
26.14
10
31.25
p=1.000000*
50
27.03
Splenectomy
3
1.96
1
3.13
p=1.000000*
4
2.16
Drainage, peritoneal lavage
24
15.69
10
31.25
p=0.164041*
34
18.38
Enterectomies
2
1.31
1
3.13
p=0.485067*
3
1.62
p†
p<0.0001**
Total
211
82.42
52
100.00
263
85.39
p<0.05 shows a statistically signi cant di erence between the groups studied
* Fisher’s exact test
** Chi-square test
*** EBD- external biliary drainage
out in 44.44% of the cases, enterectomies in 37.04% and
percentage than in non-diabetics (23.53%) (p=0.010013).
colectomies in
18.52%, with a statistical di erence
ere was no signi cant di erence in colectomies carried
(p=0.0131) (Table XIII). Enterectomy was carried out in
of diabetic patients (20.00% vs. 17.65%9 (p=1.000000),
60.00% of diabetic patients, with a signi cantly higher
while exploratory laparotomy was carried out almost 3
32
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
times more in the non-diabetic than diabetic (58.82%
dependent, 15.16% of which followed a mixed therapy
versus 20.00%) (p=0.009911) (Table XIII).
(OAD + insulin). We noted a signi cant percentage of
Acute pancreatitis
patients diagnosed with Diabetes mellitus on admission for
Acute pancreatitis represented 7.66% (308 patients)
acute abdomen (16.39%). As expected, para-clinical study
of the total number of cases of acute abdomen, being
demonstrated that the level of glycemia measured before
more frequent in the diabetic 10.66% (52 patients),
the surgical intervention, in the rst post-operative day and
than the non-diabetic 7.25% (256 patients) (p=0.0103).
in the subsequent period of hospitalization was higher in
Majority of the cases of acute pancreatitis were
diabetic patients than in the non-diabetic patients, with a
biliary in origin
(56.49%), the toxic and metabolic
signi cant statistical di erence of (p<0.0001). In the whole
causes comprised 20.45%, 16.23% respectively, with a
study group, the most frequent form of acute abdomen was
signi cant di erence (p<0.0001). Non-diabetic patients
that caused by peritonitis
(60.03%), followed by the
developed edematous pancreatitis with a signi cant
occlusive
(25.24%). While the vascular form, acute
di erence compared to diabetic patients, while the
pancreatitis and false acute abdomen were signi cantly
necrotic-hemorrhagic form or pancreatic abscess
more frequent in diabetic patients (p<0.05), the peritonitic
predominated in diabetic patients, without a statistical
form was more frequent in the non-diabetic (p=0.0003).
signi cance between the groups (Table XIV).
In terms of the occlusive, hemorrhagic forms and organ
e grade of operability predominated in late
torsion, there were no signi cant statistical di erences
emergency cases (55.68%). Diabetic patients had an
between the two groups (p>0.05). e grade of operability
operability grade higher than that of immediate
was statistically insigni cantly higher in the non-diabetic in
emergency
(43.75% vs.
13.07%, p=0.000195),
comparison to the diabetic (p>0.05). Postoperative morbidity
compared to the non-diabetic, whose operability grade
was present in 15.06% of patients, with the most frequent
was higher for the late emergency (59.48% vs. 37.50%,
postoperative complication being wound suppuration and
p=0.030772).
Laparoscopic
cholecystectomy
hematoma (12.58%), followed by postoperative stulas in
predominated (50.81%), followed by cholecystectomy
2.48% of cases (p<0.0001). General morbidity was seen in
(28.65%), necrosectomie
(27.03%), drainage and
22.01% of patients and was characterized by the presence
peritoneal lavage
(18.38%), cholecystectomy + EBD
of pneumonia, cardiovascular complications, acute renal
(external biliary drainage)
(13.51%), splenectomy
insu ciency, urinary tract infections, sepsis state, metabolic
(2.16%) and enterectomies (1.62%), with a signi cant
imbalance and neurological disturbances, with a statistical
statistical di erence (p<0.0001) (Table XV).
signi cance between the variables
(p<0.0001). In the
In the non- diabetic, as well as the diabetic, the
present study, the presence of morbidity prolonged the
highest mortality was recorded in the vascular forms
average duration of hospitalization by approximately 2
(11.76%, 25.00% respectively), followed by peritonitis
days in non-diabetic patients and 10.2 days in diabetic
(5.65% versus 10.94; RR=1.0593 / p=0.0105) acute
patients, as well as a stationary period in the ICU, with a
pancreatitis (8.59%, 11.54% respectively). Regardless
signi cant statistical di erence between the two groups
of the form of acute abdomen, mortality was higher in
(p<0.0001). In our study group, 238 deaths were recorded,
the diabetic than in the non-diabetic.
resulting in a general morbidity of 5.92%, signi cantly
higher in the diabetic than in the non-diabetic (9.84% vs.
Discussion
5.38%) (p=0.0018). In general, males had a higher risk of
mortality than the females. e risk of death was higher in
In our study, the majority of patients were females, in
diabetic females than in the non-diabetic females
the non-diabetic as well as well in the diabetic, resulting in
(RR=1.0585 / p=0.0047). us, diabetic patients of the
a F/M ratio of 1.6:1 and 1.4:1 respectively, with a signi cant
female sex, residing in urban areas, over 50 years of age, due
di erence (p<0.0001).
e mean age was signi cantly
to the presence of peri-, intra and post-operative
higher in the diabetic than in the non-diabetic (62.14 years
hyperglycemia had a higher risk for postoperative
versus 49.37 years) (p<0.0001). Over 60% of non-diabetic
complications, both local and general, thus increasing the
patients were between the ages of 30-69 years, while
risk of postoperative mortality, in comparison with non-
majority of those in the diabetic group (85.86%) were
diabetic patients. Highest mortality was recorded in
above 50 years of age. Clinical study showed that majority
patients with the vascular form of acute abdomen
of the diabetic patients with acute abdomen had Type 2
(16.67%), followed by acute pancreatitis
(9.09%),
Diabetes mellitus (95.90%) (p<0.0001) with a duration of
hemorrhagic acute abdomen
(6.71%) and peritonitic
evolution of diabetes over 10 years (34.43%), treated with
(6.21%). ere were no deaths recorded in cases of organ
oral anti-diabetic drugs (57.79%). 25.82% were insulin-
torsion.
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
33
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
In diabetic patients postoperative morbidity was
2.
Sue Kirkman M, Briscoe VJ, Clark N, et al.
recorded in 36.27% of patients operated, a signi cantly
Development Conference on Diabetes and Older Adults.
higher percentage than in non-diabetic patients (14.43%)
Diabetes in older adults: a consensus report. J Am
(p<0.0001). e relative risk is a signi cant di erence of
Geriatr Soc 2012;60(12):234256.
1, therefore there is an increased risk of postoperative
3.
American Diabetes Association. Standards of medical
morbidity in diabetic patients compared with non-
care in diabetes-2012. Diabetes Care 2012;35 Suppl
diabetic patients for wound suppuration, hematoma, and
1:S11-63.
intestinal stula. Regarding general morbidity, there is a
4.
Inzucchi SE, Bergenstal RM, et al. Management of
remarkably high risk of sepsis, metabolic imbalance,
hyperglycaemia in type 2 diabetes: a patient-centered
pneumonia, urinary tract infections, acute renal
approach. Diabetologia 2012;55(6):1577-96.
insu ciency and cardiovascular complications in diabetic
5.
Noordzij PG, Boersma E, Schreiner F, et al. Increased
patients in comparison to the non-diabetic (p<0.05).
preoperative glucose levels are associated with perioperative
It is estimated that 25% of patients with diabetes
mortality in patients undergoing noncardiac, nonvascular
mellitus will require surgical intervention [9].
e rate
surgery. Eur J Endocrinol 2007;156:137-142.
of mortality in patients with diabetes mellitus was
6.
Krentz AJ, Nattras M. Acute metabolic complications of
estimated to be 5 times higher than in non-diabetic
diabetes. In: Pickup JC, William G. Textbook of
patients, due to multiple organ failure [10]. Chronic
diabetes. Black well Science Ltd 2003, 32.10-32.22.
complications which result in microangiopathy
7.
Pătrașcu T, Doran H, Catrina E, et al. Particularită i
(retinopathy, nephropathy and neuropathy) and
ale chirurgiei la diabetici, Ed. Niculescu, 2005.
macroangiopathy (atherosclerosis) directly increase the
8.
Păcescu E, Bugă C, Pătrașcu T, Brezean I, Doran H.
need for surgical interventions and surgical
Di cultă i de diagnostic în abdomenul acut peritonitic
complications due to infections and vasculopathy [11].
la bolnavul diabetic, Chirurgia 1999;6(94):485-93.
Infections represent
66% of postoperative
9.
Blomgren KB, Sundström A, Steineck G, Wiholm
complications and a quarter of peri-operative deaths in
BE. Obesity and treatment of diabetes with glyburide
patients with DM. Data suggests impaired leukocyte,
may both be risk factors for acute pancreatitis. Diabetes
including modi cation of chemotaxic and phagocytic
Care 2002;25(2):298-302.
activity
[12].
e development of perioperative
10.
Smiley DD, Umpierrez GE. Perioperative glucose
hyperglycemia proved to be a sensitive predictor of
control in the diabetic or nondiabetic patient, South
nosocomial infections in small observational studies in
Med J 2006;99:580-589; quiz 590-591.
general surgery. A strict glycemic control is important to
11.
Umpierrez GE, Isaacs SD, Bazargan N, You X, aler
minimize infection [13].
LM, Kitabchi AE. Hyperglycemia: an independent marker
In addition to the infectious postoperative
of in-hospital mortality in patients with undiagnosed
infections, myocardial ischemia is increased among
diabetes. J Clin Endocrinol Metab 2002;87:978-982.
patients with DM undergoing cardiac and non-cardiac
12.
Ramos M, Khalpey Z, Lipsitz S, et al. Relationship of
surgical interventions
[14]. Data from observational
perioperative hyperglycemia and postoperative infections
studies suggests that in surgical patients with or without
in patients who undergo general and vascular surgery.
diabetes mellitus, a strict control of glycemic positively
Ann Surg 2008;248:585-59116.
a ects morbidity and mortality in a variety of surgical
13.
Bailey IS, Rhodes M, O’Rourke N, Nathanson L,
populations
[15,16]. Although intensive glycemic
Fielding G. Laparoscopic management of acute small
control continues to be the standard of care in diabetic
bowel obstruction. Br J Surg 1998;85(1):84-7.
patients, there is a risk of secondary hypoglycemia which
14.
Dragomirescu C, Li escu M, Iordache N, et al.
poses a risk to the bene t in morbidity and mortality.
Conversions and reinterventions in laparoscopic
e goal is to nd a balance in this situation, a reason
cholecystectomy. Chirurgia 1998;93(5):279-84.
for which current guidelines recommend a less strict
15.
Pant N, Kadaria D, Murillo LC, Yataco JC, Headley
glycemic control, usually between 80-150 mg/dL [17].
AS, Freire AX. Abdominal Pathology in Patients With
Diabetes Ketoacidosis. Am J Med Sci 2012 Jan 20.
16.
Haap M, Artunc F, Haa CS, Horger M, Teichmann R,
References
Riessen R. A rare di erential diagnosis of acute abdominal
pain. Dtsch Med Wochenschr 2009;134:28-29.
1. Krinsley JS. E ect of an intensive glucose management
17.
Kimura W, Mizutani M, Fuse A. Problems and therapeutic
protocol on the mortality of critically ill adult patients.
strategy for emergency operation of the abdomen in the aged.
Mayo Clin Proc 2004;79(8):992-1000.
Nihon Ronen Igakkai Zasshi 2004;41(6):660-5.
34
Dejeu et al
ORIGINAL ARTICLES
NEWS IN THE TREATMENT OF HEPATIC HYDATID CYST
Adela Camelia Nichita1, Adrian Maghiar2, Daniela Dinulescu3, Teodor Traian Maghiar4
1Department of Radiology-Imagistic Medicine, “Dr. Pop Mircea” Marghita Municipal Hospital, 2Department of General
Surgery, Surgical Disciplines, 3Department of Radiology-Imagistic Medicine, Department of Morfologic Disciplines,
4Department of Morfologic Disciplines, Pelican Hospital Oradea, a liated to Faculty of Medicine and Pharmacology,
Oradea University, România
Address for correspondence:
Dr. Adela Camelia Nichita
Faculty of Medicine and Pharmacology, Oradea University, România
10, 1 Decembrie Pl, 410073, Oradea, Romania
Tel: +40744400774
Email: adela_abrudan@yahoo.com
Received: 05.08.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 35-42
Abstract
Results: Of the 120 patients admitted with suspected
hydatid cyst, 74 were women, 46 were male, the peak
is study is an analysis of the modern treatment of
incidence of the disease was the age group 31-40 years,
hepatic hydatid cyst, selecting the therapy that gives us
followed by 41-50 years (p<0.05). Comparing the two
the lowest morbidity, mortality and recurrence of liver
groups of patients from the point of view of surgical
hydatid disease.
procedures, partial perichistectomia Lagrot was performed
Materials and Methods:
is observational,
to patients treated laparoscopically (p=0.0010), and left
prospective cohort study was conducted during 2007-
lobectomy was performed to the classic surgery treated
2013, on a total of 120 patients admitted with the
patients
(p=0.0468). From the point of view of
diagnosis of hydatid cyst , and tracked the incidence of
postoperative development, morbidity and disease
hepatic hydatid disease based on age, sex, the area of
recurrence was higher in patients receiving conservative
origin, clinical and paraclinical evaluation, as well as the
surgery, showing a high risk of external biliary stula
type of treatment instituted: medical, classical surgery
compared to patients treated laparoscopically and with
(radical or conservative) and laparoscopic surgery. Out
radical surgery. Death occurred in four patients treated
of the 120 patients, 20 were asymptomatic, receiving
with classic surgery, due to general postoperative
drug treatment only, and 100 had symptomatic hepatic
complications, pulmonary embolism and sepsis with
hydatid cyst, to which treatment was surgical and
multi-organ failure.
ese complications have led to
medical. ey were divided into two groups: Group A
increased patient hospitalization period to 60 days.
e
- 78 (78%) patients eligible for classical surgery, of
correlation coe cient between classic and laparoscopic
which 38 (48.72%) underwent conservative surgery and
surgery and external biliary stula occurrence, as a
40 (51.28%) that had radical surgery and Group B - 22
common complication after surgery, shows a moderate
(22%) patients eligible for laparoscopic treatment
correlation between these variables.
(uncomplicated cyst, of medium size, corticated and
Conclusions: Morbidity and recurrence rate were
located in the anterior hepatic segments (II-VI segments
higher in patients who received conservative surgery, as
following the classi cation of Couinaud).
they presented a higher risk of external biliary stula,
News in the Treatment of Hepatic Hydatid Cyst
35
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
compared with patients who underwent radical surgery.
of hepatic hydatid cyst. e study represents collaboration
Laparoscopic surgical approach is safe and e ective for
between the Department of Surgery I within the County
treating patients with uncomplicated medium-sized
Emergency Clinical Hospital Oradea, the Department
corticated hydatid cyst and preferably located in the
of Surgery within Pelican Hospital Oradea and the
anterior hepatic segments (the II-VI segments following
Department of Radiology within the County Emergency
the classi cation of Couinaud). Considering the well
Clinical Hospital Oradea.
known bene ts of minimally invasive surgery,
Of the
120 patients,
20 were asymptomatic,
laparoscopic approach o ers a viable alternative to
receiving drug treatment, and 100 had symptomatic
conventional surgery for the treatment of hepatic
hepatic hydatid cyst, where the treatment was surgical
hydatid cysts and is worthy of being considered for
and with medicines. ey were divided in two groups:
appropriate situations. Regarding external biliary stula
Group A
-
78
(78%) patients eligible for the
occurrence, as a common complication after surgery,
conventional surgical treatment, of which 38 (48.72%)
the current study demonstrates a moderate correlation
underwent conservative surgery (surgical intervention
between this complication and the classical surgical
that preserves partially or totally the pericyst) and 40
treatment (conservative, radical) and laparoscopic.
(51.28%) underwent radical surgery
(surgical
Keywords: Hydatic hepatic cyst, surgical treatment,
intervention that completely excises the pericyst) and
Lagrot partial pericystectomy, total pericystectomy,
Group B - 22 (22%) patients eligible for laparoscopic
hepatectomy
treatment
(uncomplicated cyst, medium sized,
corticalized and located in the anterior hepatic segments
Introduction
(segments II-VI by Couinaud’s classi cation).
e informed consent was given by all patients and
e untreated hydatid cysts grow in size and
the study was approved by the internal advisory
eventually cause complications that lead to disability or
committee of the research and development activities
even death. Only in exceptional cases spontaneous
within the hospital.
healing may occur through the death of the parasite and
e open surgical approach was performed by a
cyst calci cation. For these reasons, it is generally
supra umbilical midline incision or a sub costal incision.
accepted that hepatic hydatid disease diagnosed in time
Any adhesion between the cyst and neighboring organs
should be treated as early as possible [1].
was lysed. In order to prevent secondary peritoneal
ere is still no consensus on the optimal form of
hydatidosis, the peritoneal cavity was isolated with
treatment. e modern treatment of the hepatic hydatid
wicks soaked in 20% hypertonic saline solution before
cyst varies from surgery to percutaneous drainage or
any maneuver on the hydatid cyst was performed.
medical therapy.
Parasite inactivation was performed by injecting 20%
is study is an analysis of the modern treatment of
hypertonic saline solution. After 5 minutes, the hydatid
hepatic hydatid cyst with the aim of selecting the most
content was aspirated. Starting from the puncture site,
appropriate therapy in order to obtain the lowest
the cystotomy was performed with the extraction of the
possible morbidity, mortality and recurrence. is goal
germinal membrane and daughter vesicles.
is achieved in the context of a ve-year clinical experience
In the present study total pericystectomy was
in the treatment of hepatic hydatid cyst.
performed, left lobectomy and left hepatectomy, as
e objectives pursued the comparative e ciency
radical procedures, Lagrot partial pericystectomy, as
of the radical versus conservative surgical procedures,
conservative procedure.
the feasibility, safety and e ciency of the laparoscopic
e laparoscopic approach four incisions were
treatment versus conventional surgical treatment. It was
made: a supra umbilical 10 mm incision through which
also aimed at the morbidity, mortality and recurrence
a laparoscope was inserted, another 10 mm incision in
rate of the disease, the establishment of a correlation
the epigastrum as near as possible to the cyst, being used
between the type of treatment practiced and the
as a working channel, and two
5 mm incisions
occurrence of postoperative biliary stula, complication
depending on the location of the cyst. Carbon dioxide
present in both types of treatment practiced.
was insu ated in the abdominal cavity, and any
adhesion between the cyst and the neighboring organs
Material and methods
was lysed. In order to prevent the secondary hydatidosis
wicks soaked in 20% hypertonic saline solution were
is study was conducted between 2007 and 2013
inserted through the working trocars and isolated the
on a total of 120 patients hospitalized with the diagnosis
hydatid cyst from the remainder of the peritoneal cavity.
36
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
en, a puncture needle of 5 mm diameter connected
Table I. Demographic, clinical, laboratory characteristics
to a vacuum system, punctured the hydatid cyst and
and treatment of patients su ering from hepatic hydatid cyst
aspirated a part of the content. Another vacuum cannula
TOTAL PACIENTS
120
p†
is inserted through another working trocars and
Sex
permanently maintained close to the puncture needle to
Female
74 (61.7%)
prevent any spillage of the hydatid uid. e puncture
p=0.000466*
Male
46 (38.3%)
needle once inserted in the cystic cavity is not removed
Mean age (years)
(20-30) 14
until the complete evacuation of the cystic content. is
(31-40) 54
combined with the presence of the vacuum cannula
p<0.0001**
(41-50) 36
near the puncture needle and the presence of the wicks
(51-69) 16
soaked in solicited solution around the cyst prevents the
Area
spillage of the hydatid content into the peritoneal cavity,
Urban
48 (40%)
reducing to minimum the possibility of dissemination
p=0.002907*
Rural
72 (60%)
of the hydatid uid in the peritoneal cavity and the
Clinical panel
occurrence of secondary hydatidosis.
Asymptomatic
20 (17%)
20% hypertonic saline solution was injected into
p<0.000001*
Symptomatic
100 (83%)
the cyst to inactivate the parasite. After 5 minutes the
Complicated hydatid cyst
10 (10%)
hydatid content was aspirated. Cystotomy was
p<0.000001*
Uncomplicated hydatid cyst
90 (90%)
performed, starting at the puncture site, and inspection
Cystic ultrasound classi cation£
of the pericyst cavity with the laparoscope in order to
Asymptomatic
identify possible biliocystic
stulas.
e germinal
Type I/CE1
4 (20%)
membrane, sectioned pericyst and soaked wicks were
p=0.000360*
Type II/CE3
16 (80%)
extracted into a plastic bag (endobag).
Symptomatic
e surgical procedures chosen for the laparoscopic
Type II/CE3
6 (6%)
treatment of the residual cavity were Lagrot partial peri
T
ype III/CE2
64 (64%)
p<0.0001**
cystectomy (and drainage of the remaining cavity) and
Type IV/CE4
30 (30%)
total peri cystectomy.
Location of the cysts treated surgically according to
In order to prevent any possible secondary
Couinaud’s classi cation
hydatidosis through intraoperative contamination, all
Segments II-IV
30 (30%)
patients were treated with albendazole (10 mg/kg/day)
Segments V-VI
36 (36%) p=0.6570**
for 7 days preoperatively and for 3 months postoperative,
Segment VIII
34 (34%)
monitoring the hepatic transaminases.
Treatment
e methods of statistical analysis were the Chi-
Classic surgical
78 (78%)
p<0.000001*
square test, Fisher’s exact test, Comparison of means
Laparoscopic
22 (22%)
test, Comparison of proportions test, Relative risk test
* Fisher’s exact test
and calculation of the correlation coe cient using the
** Chi-square test
medical statistics software MedCalc® version 12.2.1.0
†p<0.05 shows a statistically signi cant di erence between the
groups studied
(MedCalc® Software, Mariakerke, Belgium).
£ Gharbi ultrasound classi cation / WHO ultrasound classi cation
of the hydatid cyst
Results
Of the 120 patients hospitalized with the suspicion
features occurred in patients (17%) in an early stage of
of hepatic hydatid cyst, 74 were women and 46 were
the disease, the cystic lesion being discovered accidentally
men, 48 came from urban areas and 72 from rural areas,
on a routine ultrasound or radiographic examination
with statistically signi cant di erence, p<0.05.
(p<0.000001).
e incidence of complicated hepatic
e maximum incidence of the disease was in the
hydatid cyst in patients included in the study was 10%
age group of 31-40 years, followed by 41-50 years,
(Table I).
a ecting young people who by the nature of the work
e abdominal ultrasound had an important role in
they practice come into contact with the disease vector
diagnosing the hepatic hydatid cyst. e presence of the
(Table I).
symptoms is directly proportional to the degree of
From the clinical point of view, most patients (83%)
ultrasound lesion.
us, asymptomatic patients, being
had clinical symptoms, the absence of the clinical
in an early stage of disease, with cystic lesions of Type I/
News in the Treatment of Hepatic Hydatid Cyst
37
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
In Group A 78 (78%) patients were classically
surgically treated, 38 (48.72%) conservatively, with the
localization of the hydatid cysts in segments II-IV - 10
(26%), segments V-VI - 14 (37%), segments I-VII - 10
(26%) and segment VIII - 4 (11%) (p=0.0670), and 40
(51.28%) radically, the localization of the hydatid cysts
being in segments II-IV - 12 (30%), segments V-VI -
18 (45%), segments I-VII - 6 (15%) and segment VIII
- 4 (10%) (p=0.0011).
e patients in Group B - 22 (22%) underwent
Figure 1. Surgical treatment depending on the location
surgery by laparoscopic approach. It was performed in
of the cyst in the liver segments
patients with uncomplicated hydatid cyst, located
predominantly in the liver segments V-VI -12 (55%),
II-IV - 8 (36%) and segment VIII -2 (9%) (p=0.0001)
CE1 and Type II/CE3, received medical treatment with
(Figure 1).
Albendazole (Zentel) 10 mg/kg/day for three months,
e hydatid cysts subject to laparoscopic surgery
unlike symptomatic patients where the evolutionary
were Type II/CE3 and Type III/CE2 young and
stage of the cystic lesions was more advanced, being
uncomplicated cysts, located predominantly in the
predominant Type III/CE2
(64%), who underwent
marginal liver segments II-VI, while the classic surgical
surgical treatment associated with drug treatment. It
treatment has been practiced in cysts of Type III/CE2,
consisted of classical conservative surgical procedures
followed by Type IV/CE4 (Table II).
(Lagrot partial peri cystectomy) or radical (total peri
CE2 WHO (World Health Organization) stage is
cystectomy, left hepatectomy, left lobectomy) and
characterized by daughter cysts with the appearance of a
laparoscopic surgical procedures, depending on the
“honeycombed”, which may partially or completely ll
location and polymorphism of the lesions.
the fertile uni locular mother cyst, and corresponds to
Analyzing the distribution of the patients with
Gharbi Type III, a loculated uid collection, given by a
hydatid cyst in the two groups according to the liver
process of internal vesiculation triggered by a mechanical,
segmentation, we can observe that in group A the
chemical or infectious aggression of the cyst.
distribution of the cysts is relatively well proportioned
CE3 WHO transitional stage is characterized by
in patients with conservative surgical treatment versus
cysts that degenerate, but still contain viable protoscoleces,
those who underwent radical surgical treatment. Here
oating membranes in the cystic uid, and corresponds
the cysts were located in the marginal segments of the
to Gharbi Type II, a uid collection +/- hydatid sand with
liver, allowing the proper technique and avoiding the
dedoubled wall and onset of detachment of the hydatid
risk of interception of major biliary vascular pedicles.
membrane (partial or total detachment).
Table II. Surgical treatment according to Gharbi /WHO ultrasound classi cation
and mean size of the hydatid cyst (cm)
Total patients
Group A
Group B
p†
100 (100%)
78 (78%)
22 (22%)
Type II/CE3
0
6 (27%)
p=0.000063*
Type III/CE2
48 (62%)
16 (73%)
p=0452202*
Type IV/CE4
30 (38%)
0
p=0.000145*
Mean size of the hydatid cyst (cm)
10.48±4.74 (2-18)
8,36±5.27 (2-15) p=0.0737**
Lagrot partial peri cystectomy
38 (48.72%)
20 (90.91%)
p=0.0010***
Total peri cystectomy
22 (28.21%)
2 (9.09%)
p=0.1160***
Left lobectomy
16 (20.51)
0
p=0.0468***
Left hepatectomy
2 (2.56%)
0
p=0.9166***
* Fisher’s exact test
** Comparison of means test
*** Comparison of proportions test
†p<0.05 shows a statistically signi cant di erence between the groups studied
£ Gharbi ultrasound classi cation / WHO ultrasound classi cation of the hydatid cyst
38
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
partial peri cystectomy performed in 90.91% of the
patients treated laparoscopically compared to 48.72%
of those treated by classical surgery, showing a
statistically signi cant di erence (p=0.0010), and left
lobectomy performed in 20.51% of the patients treated
by the classic surgery compared to those treated
laparoscopically (p=0.0468) (Figure 2).
In terms of postoperative evolution, we can see that
the morbidity rate was signi cantly higher among the
patients subject to classic surgical treatment versus those
treated laparoscopically (surgical complications 82% vs.
Figure 2. Distribution of patients according
18%, p<0.0001 / general complications 37% vs. 0,
to the surgical procedures
p=0.0018), the statistical analysis showing a higher
incidence of wound complications
(seromas and
abscesses), followed by external biliary stula, abscess of
CE4 WHO stage corresponds to an inactive hydatid
the residual cavity and hemorrhage (Table III).
cyst, characterized by an advanced degeneration, probably
Death occurred in four of the patients subject to
infertile, with heterogeneous appearance, with little or no
classic surgical treatment due to general postoperative
daughter cysts, having as correspondent Gharbi Type IV
complications, pulmonary embolism and sepsis with
- formation of solid echo structure, heterogeneous
multiple organ failure. ese complications have lead to
appearance, corresponding to a reshaped, old cyst.
the increment of the hospitalization period of the patient
e hydatid cysts treated by classic surgery ranged
to 60 days, statistically signi cant (p<0.0001) compared
in size between 2-18 cm, with a mean of 10.48±4.74
to the group of patients treated laparoscopically (Table
with no statistically signi cant di erence compared to
III). Regular, clinical and imaging monitoring at 3, 6
those treated laparoscopically, where the size ranged
and 12 months after surgery, hasn’t recorded recurrences
between 2-15, with a mean of 8.36±5.27 (Table II).
of the hydatid disease in patients treated laparoscopically,
Comparing the surgical procedures, the results were
unlike the patients treated by classic surgery who had
similar between the two study groups, except for Lagrot
relapse rate of 5% (Figure 3).
Table III. Postoperative morbidity and mortality in patients subject to surgery
for hepatic hydatid cyst
Total patients
Group A
Group B
p†
100 (100%)
78 (78%)
22 (22%)
Surgical complications
p<0.0001*
Wound complications
30 (38%)
0
p=0.0015*
External biliary stula
24 (31%)
2 (9%)
p=0.0720*
Abscess of the residual cavity
4 (5%)
2 (9%)
p=0.8483*
Hemorrhage
6 (8%)
0
p=0.3837*
General complications
p=0.0018*
Pneumonia
10 (13%)
0
p=0.1663*
Pleural e usions
14 (18%)
0
p=0.0720*
Pulmonary embolism
2 (3%)
0
p=0.9811*
Multiple organ failure
2 (3%)
0
p=0.9811*
Relapse
4 (5%)
0
p=0.6553*
Mortality
4 (5%)
0
p=0.6553*
Operative time (minutes)
82.46±23.79
87.63±26.73
p=0.3832**
(35-120)
(40-140)
Days of hospitalization
32.53±16.14
11.63±2.73
p<0.0001**
(7-60)
(7-16)
*Comparison of proportions test
**Comparison of means test
†p<0.05 shows a statistically signi cant di erence between the groups studied
News in the Treatment of Hepatic Hydatid Cyst
39
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table IV. Postoperative morbidity and disease recurrence
Conservative
Radical
Group A
Relative risk
interventions
interventions
p†
78 (78%)
(IC 95%)
38 (48.72%)
40 (51.28%)
Morbidity
p=0.0016*
Hemorrhage
2 (5%)
4 (10%)
1.0526
p=0.4308**
(0.9265-1.1959)
External biliary stula
20 (53%)
4 (10%)
0.5263
p=0.0003**
(0.3706-0.7474)
Abscess of the residual cavity / subphrenic
2 (5%)
2 (5%)
0.9972
p=0.9580**
(0.8994-1.10581)
Relapse
4 (11%)
0
0.8955
p=0.0676**
(0.7956-1.008)
*Comparison of proportions test
**Relative risk test
†p<0.05 shows a statistically signi cant di erence between the groups studied
Analyzing the comparative e ciency of the radical
versus conservative surgical procedures
(intervention
that keeps partially or totally the pericyst) regarding the
morbidity rate and disease recurrence, this study
demonstrated that the morbidity rate was higher in
patients who were subject to conservative interventions
(p=0.0016), with a statistical signi cant increased risk
for external biliary stula
(p=0.0003), as well as the
disease recurrence rate, but with no statistically signi cant
di erence between the two groups (Table IV).
Figure 3. Hydatid disease recurrence rate after surgery
e bleeding complications were more frequent in
in the two groups of patients studied
patients subject to radical surgical treatment, but with
no signi cant di erence with respect to those subject to
conservative surgical treatment. Two patients subject to
conservative surgical treatment had abscess of the
residual cavity and other two subject to radical surgical
treatment had sub phrenic abscess (Figure 4).
e external biliary stula was a postoperative
complication in 20 cases subject to conservative surgical
treatment (out of 38), in 4 cases subject to radical
surgical treatment (out of 40) and in 2 cases of the 22
treated laparoscopically.
Figure 4. e postoperative relapse rate of hydatid disease is
e correlation coe cient between the conservative,
higher in patients subject to conservative surgical treatment
radical and laparoscopic surgical treatment and the
occurrence of external biliary stula, as a common
postoperative complication (r=0.5), shows a moderate
correlation between those variables (Figure 5).
Discussion
An optimal therapeutic management of the patient
with hepatic hydatid disease means a careful evaluation,
taking into account the location and number of hydatid
cysts, the presence of complications, especially biliary,
the risks and bene ts, the indications and
Figure 5. Correlation between the type of surgical treatment
and the occurrence of postoperative biliary stula
contraindications, the surgeon’s experience, before
40
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
making a decision on the type of surgery and the time of
role of laparoscopy in the management of hydatid
performing it [2,3].
disease have not been solved so far [4,15].
is study
Surgery remains the gold standard therapy [4,5] and
proves that laparoscopic surgical approach is safe and
can be carried out by classical or laparoscopic approach.
e ective for treating the patients with uncomplicated
e surgical procedures performed for hydatid cysts can
hydatid cyst, medium sized, corticalized and located
be brie y divided into radical and conservative
preferably in the anterior hepatic segments (segments
approaches. Radical procedures include peri cystectomy
II-VI by Couinaud’s classi cation). Considering the
and liver resection. However, the most common
well known bene ts of minimally invasive surgery, the
technique is total or partial cystectomy [6-9].
laparoscopic approach o ers a viable alternative to the
ese surgical procedures may be associated with
conventional surgery for the treatment of hepatic
allergic or anaphylactic reactions as well as with the risk
hydatid cysts and is worthy of being considered for
of secondary dissemination, therefore chemotherapy
appropriate situations.
with mebendazole or albendazole is indicated before
Regarding the occurrence of external biliary stula,
and especially after surgery.
e treatment with
as a postoperative common complication, this study
albendazole seems to be more e cient due to its better
demonstrated the existence of a moderate correlation
penetration and absorption. Gil Grande et al. showed
between this complication and classic
(conservative,
that albendazole (10 mg/kg/day) sterilize the cyst in
radical) and laparoscopic surgical treatment.
72% of the cases after the rst month of treatment and
in 94% of the cases after 3 months of treatment [10,11].
In the present study the treatment of hepatic
References
hydatid cyst was medical, classic surgical, conservative
(Lagrot partial peri cystectomy) or radical (total peri
1.
Eckert J, Deplazes P. Biological, epidemiological, and
cystectomy, left hepatectomy, left lobectomy) and
clinical aspects of echinococcosis, a zoonosis of increasing
laparoscopic depending on the location and
concern. Clin Microbiol Rev 2004;17(1):107-35.
polymorphism of the lesions. Analyzing the distribution
2.
Magistrelli P, Masetti R, Coppola R, Messia A, Nuzzo
of the patients with hydatid cyst in the two groups
G, Picciocchi A. Surgical treatment of hydatid disease of
according to liver segmentation, in group A the
the liver. A
20-year experience. Arch Surg
distribution of the cysts was relatively well proportioned
1991;126(4):518-22; discussion 523.
in patients with conservative surgical treatment versus
3.
Zaouche A, Haouet K. Traitement chirurgical des
those who underwent radical surgical treatment. Here
kystes hydatiques du foie. EMC, Techniques
the cysts were located in the marginal segments of the
chirurgicales, Appareil digestif. Elsevier Masson
;40-
liver, therefore allowing the proper technique and
775.
avoiding the risk of interception of major biliary vascular
4.
Hasan HM, El-Sayed OM. Laparoscopic treatment of
pedicles.
e laparoscopic surgical treatment was
liver hydatid cyst. J Med Biomed Sci 2010;1:47-51.
performed in patients with uncomplicated hydatid cyst
5.
Yagci G, Ustunsoz B, Kaymakcioglu N, et al. Results
located predominantly in the marginal liver segments
of surgical, laparoscopic, and percutaneous treatment for
II-VI.
hydatid disease of the liver: 10 years experience with 355
In general, it is considered that radical surgery is
patients. World J Surg 2005;29(12):1670-9.
accompanied by a higher intraoperative risk with a
6.
Belghiti J, Benhamou JP, Houry S, Grenier P, Huguier
lower recurrence rate, while conservative surgical
M, Fékété F. Caustic sclerosing cholangitis. A
approach has a lower perioperative risk but a higher
complication of the surgical treatment of hydatid disease
recurrence rate [12]. In our study also the morbidity
of the liver. Arch Surg 1986;121(10):1162-5.
rate and disease recurrence was higher in patients who
7.
Sa oleas M, Misiakos E, Manti C, Katsikas D,
were subject to conservative interventions, the same
Skalkeas G. Diagnostic evaluation and surgical
showing a high risk for external biliary stula, compared
management of hydatid disease of the liver. World J
with the patients who were subject to radical surgical
Surg 1994;18(6):859-65.
treatment. Also the mortality rate was signi cantly
8.
Morris DL, Dykes PW, Dickson B, Marriner SE,
higher among the patients treated by classic surgery
Bogan JA, Burrows FG. Albendazole in hydatid disease.
compared to those treated laparoscopically.
Br Med J (Clin Res Ed) 1983;286(6359):103-4.
Several reports have con rmed the possibility of
9.
Queiroz-Medeiros M, Menezes-Silva A, Raposo-
performing laparoscopic surgery for the hepatic hydatid
D’Almeida, et al. Surgical treatment of hepatic hydatid
disease [4,13,14], although controversies regarding the
disease. European IHPBA Congress, Hamburg 97,
News in the Treatment of Hepatic Hydatid Cyst
41
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Monduzzi editore, International Proceedings
cysts. Aspiration and alcohol injection under sonographic
Division, Bologna 1997;229-33.
guidance. Gastroenterology. 1990;98(5 Pt 1):1366-8.
10. Gil-Grande LA, Boixeda D, Ledo L. Tratamiento
13. Sağlam A. Laparoscopic treatment of liver hydatid cysts.
actual de la hydatidosis humana. Enferm Infect
Surg Laparosc Endosc 1996;6(1):16-21.
Microbiol Clin 1987;5:627-32.
14. Ertem M, Karahasanoglu T, Yavuz N, Erguney S.
11. Gil-Grande LA, Rodriguez Caabeiro F, et al.
Laparoscopically treated liver hydatid cysts. Arch Surg
Randomised controlled trial of e cacy of albendazole in
2002;137(10):1170-3.
intraabdominal
hydatid
disease.
Lancet
15. Bickel A, Daud G, Urbach D, Le er E, Barasch EF,
1993;342:1269-72.
Eitan A. Laparoscopic approach to hydatid liver cysts. Is
12. Filice C, Pirola F, Brunetti E, Dughetti S, Strosselli M,
it logical? Physical, experimental, and practical aspects.
Foglieni CS. A new therapeutic approach for hydatid liver
Surg Endosc 1998;12(8):1073-7.
42
Nichita et al
ORIGINAL ARTICLES
COMPARISON BETWEEN THE CLASSIC SURGICAL METHODS AND
THE LAPAROSCOPIC ONES IN THE BENIGN TUBO OVARIAN
PATHOLOGY
Nicolae Babău1, Marius Sebastian Teodorescu2
1Clinic of General Surgery II, Oradea Emergency County Clinical Hospital, Faculty of Medicine and Pharmacy Oradea,
2Clinic of Surgery I, Timișoara Emergency County Clinical Hospital, University of Medicine and Pharmacy ”Victor
Babes”, Timișoara, România
Address for correspondence:
Dr. Nicolae Babău
Faculty of Medicine and Pharmacy Oradea
10, 1 Decembrie Pl, 410073 Oradea, Romania
Phone: +40758433533 / +40770715527
E-mail: nicolae.babau@gmail.com
Received: 05.08.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 43-53
Abstract
abscesses and
60 tubal pregnancies) were surgically
treated by laparotomy. Both groups were compared
Introduction:
e pathology of the tubo-ovarian
considering the demographic characteristics, the surgical
area is very complex, in consequence so is the therapeutic
and pathological indications, the operation indices, and
management, the medication approach and the surgical
morbidity and hospitalization factors.
one, these being very varied, not mentioning that it must
Results: Analyzing the operation indices we
be personalized and having the main focus on age,
concluded that the surgery time was in average 90, 81
clinical status and the wishes of the patient who needs to
minutes for laparoscopy, as compared to laparotomy,
be properly informed. During the last years the
where it was in average 81, 16 minutes (p<0.0001). Intra-
laparoscopic surgery has gained momentum in the
surgery blood loss was signi cantly lower in the batch of
genital sphere. Many of the previously performed
patients treated by laparoscopy than of those treated by
procedures as traditional abdominal and vaginal surgeries
laparotomy (78±41.80 vs. 157±84.59; p<0.0001). e
are feasible and even easy to do through laparoscopy.
lowest percentage of oxygen saturation was of
99%,
e aim of this study is to assess the feasibility,
without signi cant di erences between batches. Cystitis
safety and e ciency of the laparoscopic treatment versus
prevailed in patients treated by laparoscopy, while the
the conventional laparotomy in the benign pathology of
pelvic infection and the infection of the surgical wound
the tuboovarian region.
were frequent in patients treated by laparotomy (p<0.05).
Materials and methods: e study was carried out
ree patients needed blood transfusions after a ruptured
on a number of 1238 cases of benign pathology in the
ectopic pregnancy, one being treated by laparoscopy and
tuboovarian area, out of which 636 cases (520 benign
two by laparotomy.
e post-operational parenteral
ovarian tumors, 28 adnexal torsions, 28 tuboovarian
dosage of analgesic and that of antiemetic were
abscesses and
60 tubal pregnancies) were surgically
signi cantly lower after laparoscopy as compared to
treated by laparoscopy and
602 cases
(436 benign
laparotomy (p<0.0001). Feverish morbidity was found in
ovarian tumors, 12 adnexal torsions, 94 tuboovarian
19 patients treated by laparoscopy as compared to 139
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
43
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
patients treated by laparotomy
(p<0.0001). Hospital
saturation during the surgical intervention, the intra
indices show a postsurgical hospitalization period and a
and post-operational complications, feverish morbidity,
postsurgical recovery period signi cantly shorter in
the postsurgical hospitalization period and the
patients treated by laparoscopy than in patients treated by
postsurgical recovery period.
laparotomy (p<0.0001).
Conclusions:
e foregoing study demonstrates
Materials and methods
feasibility, safety and e ciency of the laparoscopic
treatment in comparison with the conventional
is observational, retrospective and cohortative
laparotomy in the pathology of the benign tuboovarian
study was carried out during 2000-2012, on 1,238 cases
region
of benign tuboovarian pathology, admitted at
e
Keywords: Laparoscopy, laparotomy, tuboovarian
Emergency County Clinical Hospital, Surgery II section
benign pathology
from Oradea.
Inclusion criteria: age over
18, benign ovarian
Introduction
tumors, ectopic pregnancies with stable vital signs,
adnexal torsion, tuboovarian abscess, free adnexa or
e pathology of the tuboovarian region is complex
ones that may be mobilized under safe conditions
and thus, the therapeutic, medication and surgical
through laparoscopy, hemodynamic stability and
management should be individualized, focusing on age,
adequate surgical eld exposure (lack of adhesions).
clinical status and the patient’s wishes, if informed
Exclusion criteria: age fewer than 18 and signs of
properly.
tubal or ovarian malignancy.
e surgical indications
Due to the importance of the ovary in the hormonal
were benign ovarian tumors, adnexal torsions, tuboovarian
balance and the reproduction function in young women,
abscess or ectopic pregnancy with stable vital signs.
it is obvious that the conservative surgical techniques
All patients had a body mass index <30 kg/m2. In
have priority whenever possible.
cases of ovarian tumors a careful selection was made
In the last years, surgical laparoscopy gained
based on the disease history, the age of the patient,
momentum in the surgery of the genital zone. Many
clinical ndings and ultrasound, as well as on the seric
procedures done before as traditional abdominal and
determination of CA-125 marker. As for patients in
vaginal operations are feasible or even easy to do by
menopause the speci city of this test is reduced, in case
laparoscopy. e basic technique is largely described in
of an intra-surgical malignancy suspicion, tissue for the
the specialty literature [1].
e multiple advantages of
microscopic extemporaneous exam was taken.
e
the methods are: reducing the intra-surgical blood loss,
positive result imposed the continuation of the surgery
minimizing formation of adhesions, reducing the
by surgical stadialization laparotomy. In case the
hospitalization period, of the postsurgical pain and of
malignancy was diagnosed after the laparoscopic surgery,
the post-operational recovery period. Beside these, as
the surgical treatment for cancer was realized in one
compared to laparotomy, it also has downsides that
week. After general anesthesia a laparoscopic
limit its potential: exposure of the surgical eld may be
examination of the pelvis and the superior abdomen was
reduced, the instruments are small and can be used only
performed for diagnosis. e ovary laparoscopic surgery
by x ports and the capacity to manipulate pelvic viscera
was performed when the inclusion criteria were ful lled.
is limited. In some cases the hospitalization costs
e research group of this study comprised 636
increase, despite the short period of staying in hospital,
patients out of which 520 had benign ovarian tumors,
due to the prolonged time of stay in the surgery room
28 had adnexal torsions, 28 tuboovarian abscesses and
and to the use of more expensive devices and surgical
60 had ectopic pregnancies. e control batch was built
equipments. Ability, training and proper experience are
from cases treated in that period, with a surgical
needed to mitigate complications. e surgical time is
di culty degree with indication for laparotomy. ese
comparable with that of the laparotomy [2,3].
have been retrospectively evaluated for comparison: 602
e aim of this study is to assess the feasibility,
cases in which 436 had benign ovarian tumors, 12 had
safety and e ciency of the laparoscopic treatment versus
adnexal torsions, 94 had tuboovarian abscesses and 60
the conventional laparotomy in the benign pathology of
had ectopic pregnancies.
the tuboovarian region, following as postsurgical
e postsurgical recovery was de ned as the time
parameters: the surgery time, the postsurgical dosage of
(in days) needed for the patient to resume their daily
antiemetic, the postsurgical parenteral dosage of
routine or normal work routine. Antibiotic prophylaxis
analgesic, blood loss, the lowest percentage of oxygen
was not used routinely, except in tubo-ovarian abscesses.
44
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Complications were de ned as events which called
Table I. Distribution of benign tubo-ovarian pathology
cases depending on the anatomical seat
for active treatment or prolonged hospitalization.
Feverish morbidity was de ned as fever >38°C, measured
Benign tubo-ovarian pathology (n=1238)
twice at an interval of 24 hours post surgically, except
Fallopian tube
for the rst
24 hours after surgery. After the clinic
Ectopic pregnancy
120 (9.69%)
p†
reevaluation visit after 4 weeks postsurgical, the patients
Ovary
956 (77.22%)
went back to their normal activities.
Functional cyst
129 (13.49%)
e assessed variables were: age, parity, pre-
Endometriotic cyst
292 (30.54%)
menopause, menopause, body mass index, the diameter
Dermoid cyst
267 (27.93%)
of the ovarian cyst, the diameter of the tuboovarian
Mucinous cyst
84 (8.79%)
abscess, use and duration of use of Intrauterine Device
Serous cyst
97 (10.15%)
p<0.0001*
(IUD), surgical and pathological indications, surgery
Parovarian cyst
22 (2.30%)
time, the antiemetic post-operational dosage, the
Fibroma
28 (2.93%)
analgesic parenteral post-operational dosage, blood loss,
Others (hydrosalpinx/
37 (3.87%)
the lowest percentage of oxygen saturation during the
simple cyst)
surgical intervention, intra and postsurgical complications,
Tube and ovary
feverish morbidity, postsurgical hospitalization period
Tuboovarian abscess
122 (9.85%)
and the postsurgical recovery period.
Adnexal torsion
40 (3.23%)
e data have been collected retrospectively from the
p†
p<0.0001*
observation sheets, entered and processes with the
†p<0.05 proves a statistically signi cant di erence between studied
groups
Microsoft® Excel® 2010 software (Microsoft® Corporation,
* Chi-square test
USA), this being the basis of the statistic study.
** Fisher’s exact test
As statistic analysis methods were: the Chi-square
test, the Fisher’s exact test, Comparison of means test,
Comparison of proportions test, Relative risk test and
hydrosalpinx, simple cyst, ovarian
broma and
calculation of the correlation coe cient using the
parovarian cyst.
medical statistic software MedCalc® version 12.2.1.0
e 1238 cases of benign tuboovarian pathology
(MedCalc® Software, Mariakerke, Belgium).
were divided in two groups:
e study was approved by the internal approval
e study group (Group S) - formed of 636 patients
commission for research and development works within
(520 benign ovarian tumors, 28 adnexal torsions, 28
the hospital. All patients were informed of the risks and
tuboovarian abscesses and
60 tubal pregnancies)
complications, including the chances to converse
surgically treated by laparoscopy.
laparoscopy to laparotomy and were requested to sign
e control group (Group C) - formed of 602 cases
an informed consent form.
of benign tuboovarian pathology (436 benign ovarian
tumors, 12 adnexal torsions, 94 tuboovarian abscesses
Results
and 60 tubal pregnancies), matching as indications,
procedure, surgical di culty degree for laparotomy.
1,238 cases with benign pathology in the
Both groups were compared as to the demographic
tuboovarian sphere, admitted to the Surgery II section
characteristics, surgical and pathological indications
of the Emergency County Clinical Hospital from
(Table II).
Oradea were studied. e benign tuboovarian pathology
Age, as an epidemiologic factor, is of great
included: benign tubal pathology (ectopic pregnancy),
importance in the tuboovarian pathology, some of the
ovarian (benign ovarian tumors) or tuboovarian (adnexal
conditions from this sphere are characteristic to certain
torsions, tuboovarian abscesses) (Table I). Analyzing the
ages, being in uenced by hormonal changes and by
statistic results we can observe that most of the admitted
sexual habits. In our study the age average of the patients
patients had benign ovarian tumors (77.22%), followed
with tuboovarian pathology was around 34-35 years
by tubo-ovarian abscess, ectopic pregnancy and adnexal
with an age interval between
17-58 years, with no
torsion (p<0.0001). Among the benign ovarian tumors,
statistically signi cant di erences between the two
the endometriotic cyst was most frequent (30.54%),
studied batches. (Table II).
e body mass index was
followed by the dermoid, functional, serous and
<30 kg/m2 in all patients. e origin of patients from
mucinous cysts, with a signi cant statistic di erence
urban or rural premises is not an indicator for
(p<0.0001). A small percentage of the patients had
conclusions.
e assignment of cases does not attest a
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
45
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Table II. Demographic, clinical and paraclinical characteristics
Group S
Group C
Dates
p†
n=636
n=602
Age (years)
(17-56) 34.8±8.3
(20-58) 34.5±5.8
p=0.4544*
urban
312
289
p=1.000000**
Originating
rural
324
313
p=1.000000**
Parity
(1-3) 2.1±1.2
(1-3) 2.0±1.1
p=0.1211*
Fertile period
584
572
p=0.029359**
Menopause
52
30
p=0.029359**
Body mass index (kg/m2)
21.2±2.6
21.4±2.5
p=0.1617*
Ultrasound diameter of the ovarian cyst (cm) (average)
(4-5) 4.48±0.5
(4-12) 7.98±2.53
p<0.0001*
Ultrasound diameter of the abscess (cm) (average)
(4-7) 5.58±1.09
(7-10) 8.54±1.12
p<0.0001*
p<0.0001****
Use of IUD*
9
58
RR=1.0910
Duration for the use of IUD (year)
(2-5) 3.52±1.13
(5-10) 7.40±1.70
p<0.0001*
Surgical Indications
Pelvic mass
137 (21.5%)
149 (24.75%)
p=1.000000**
Dysmenorrhea
117 (18.4%)
142 (23.59%)
p=1.000000**
Pelvic acute pain
574 (90.3%)
543 (90.20%)
p=1.000000**
Pelvic chronic pain
62 (9.7%)
59 (9.80%)
p=1.000000**
Menstrual disorders
78 (12.2%)
88 (14.62%)
p=1.000000**
Pelvic adhesions (mild - moderate)
69 (10.8%)
38 (6.31%)
p=0.004591**
p†
p<0.0001***
p<0.0001***
Benign Pathology
Ovarian
520
436
p=1.000000**
Functional cyst
85 (16.3%)
44 (10.2%)
p=1.000000**
Endometriotic cyst
136 (26.2%)
156 (35.8%)
p=1.000000**
Dermoid cyst
104 (20%)
163 (37.3%)
p=1.000000**
Mucinous cyst
67 (12.8%)
17 (3.9%)
p=0.000001**
Serous cyst
67 (12.8%)
30 (6.9%)
p=0.002479**
Paraovarian cyst
22 (4.2%)
0 (0%)
p=0.000002**
Fibroma
16 (3.1%)
12 (2.8%)
p=0.848527**
Others (hydrosalpinx / simple cyst)
23 (4.6%)
14 (3.1%)
p=0.400941**
p†
p<0.0001***
p<0.0001***
Fallopian tube
Ectopic pregnancy
60 (9.44%)
60 (9.39%)
p=1.000000**
Adnexal torsion
28 (4.4%)
12 (1.87%)
p=0.010123**
Tubo-ovarian abscess
28 (4.4%)
94 (14.72%)
p=1.000000**
p†
p<0.0001***
p<0.0001***
†p<0.05 proves a statistically signi cant di
erence between studied groups
* Comparison of means (t-test)
** Fisher’s exact test
*** Chi-square test
**** Relative risk
statistically signi cant di erence
between batches.
All patients
were paraclinically investigated
by
(Table II).
abdominal and
transvaginal ultrasound and color
e assignment of patients
with tuboovarian
Doppler. In cases with ovarian cyst or tubo-ovarian
pathology depending on the hormonal status was done
abscesses, the dimension was taken into consideration in
in Group S, where 584 were in their fertile period and
the light of a subsequent therapeutic conduct.
e
52 at menopause, and in Group C, 572 in fertile period
indications for laparoscopy were the diameter of the
and 30 at menopause.
benign tumor formation <10 cm and the wish to preserve
46
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
fertility and the hemodynamic stability. In consequence,
the patients undergoing laparoscopic treatment had the
diameter of the ovarian cyst, and tubo-ovarian abscess net
smaller, as compared to the patients treated by laparotomy,
with signi cant di erence between batches (Table II).
As an etiologic factor, the use of an IUD increases the
risk for in ammatory pelvic disease (IPD) and, implicitly
for tuboovarian abscess. In the present study, 9 patients
treated by laparoscopy for tubo-ovarian abscess were
bearers of IUD between 2 and 5 years and 58 patients
treated by laparotomy for tuboovarian abscess were
bearers of IUD between 5 and 10 years, with statistically
signi cant di erence between batches (p<0.05).
e pathology of the tuboovarian area is complex; in
consequence the clinical background is also quite varied.
Pelvic acute pain was the main symptom dominating the
clinical background in both batches, followed by the
Figure 1. Assignment of patients in two batches
presence of a pelvic mass, dysmenorrhea, menstrual
depending on the benign tuboovarian pathology
disorders, presence of mild-moderate pelvic adhesions at
the laparoscopic diagnose exam and chronic pelvic pain,
with statistically signi cant di erences between variables
(p<0.0001), but without statistically signi cant
importance between batches. e presence of a pelvic
mass over
6-10 cm in diameter, of severe adnexal
adhesions from a laparoscopic point of view and of
hemodynamic instability, were suggestive for a severe
disease with surgical indication by laparotomy (Table II).
e indications for the laparoscopic surgery were
benign ovarian tumors, tubal pregnancy, adnexal torsion
and the tuboovarian abscess with stable vital signs. From
a statistic point of view there had been no signi cant
di erences between batches concerning the tuboovarian
Figure 2. Distribution of patients with tuboovarian abscess
pathology, except for the mucinous cyst, serous cyst,
depending on the surgical procedure
parovarian cyst and the adnexal torsion which prevailed
in the batch of patients treated by laparoscopy (Table II;
Figure 1).
e ecto dermoid cysts, the dermatoid and
Comparing the two batches, we can observe that
functional cysts represented more than half (71.93%) of
there are statistically signi cant di erences in case of the
the benign ovarian tumor pathology, followed by the
unilateral oophorectomy and salpingectomy that
serous cysts, mucinous cysts, hydropiosalpinx, simple
prevailed in the batches of patients treated by
cysts, ovarian broma and parovarian cysts (Table II).
laparotomy. Salpingotomy was only applied in patients
As to the type of surgical intervention, the
treated by laparoscopy, where tubal pregnancy was
conservatory surgical interventions predominated,
smaller than 5 cm, the gestation sack was localized in
taking into account the fertile age of the casuistic.
the ampoule or in the isthmic portion, the fertile
Radical surgical interventions were performed where the
function was needed to be preserved and the
clinical and intra-surgical background indicated it.
hemodynamic status was stable (Table III).
us, in the total batch of patients have prevailed
e hysterectomy with salpingo-oophorectomy was
cystectomies in proportion of
34.08%, followed by
a purely laparotomic surgical intervention, practiced on
salpingo-oophorectomies, salpingectomies, unilateral
patients with severe tuboovarian abscess, meaning an
oophorectomies, unilateral adnexectomies, hysterectomies
ultrasound diameter larger than 10 cm, with signs of
with salpingo-oophorectomies and salpingotomies, with
peritoneal irritation, septic state and instable
statistically signi cant di erence (p<0.0001) (Table III).
hemodynamic status (Table III; Figure 2).
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
47
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Figure 3. Distribution of patients with benign ovarian
Figure 4. Distribution of patients with ectopic tubal
tumors depending on the surgical procedure
pregnancy depending on the surgical procedure
Table III. Type of surgical intervention depending on the tubo-ovarian pathology
Group S
Group C
p†
n=636
n=602
Benign ovarian tumors
520
436
Cystectomies
230
166
p=1.000000*
Unilateral oophorectomy
35
72
p=0.000003*
Salpingo-oophorectomy
232
184
p=1.000000*
Salpingectomy
23
14
p=0.400941*
Ectopic pregnancy
60
60
Salpingectomy
12
60
p<0.000001*
Salpingotomy
48
0
p<0.000001*
Adnexal torsion
28
12
Detorsion + cystectomy
24
2
p=0.000060*
Unilateral Adnexectomy
4
10
p=0.000060*
Tuboovarian abscess
28
94
Unilateral Adnexectomy
28
26
p<0.000001*
Hysterectomy with salpingo-oophorectomy
0
68
p<0.000001*
Total
636
602
Cystectomies
254
168
p=1.000000*
Unilateral oophorectomy
35
72
p=0.000068*
Salpingo-oophorectomy
232
184
p=1.000000*
Salpingectomy
35
74
p=0.000032*
Salpingotomy
48
0
p<0.000001*
Unilateral Adnexectomy
32
36
p=0.532985*
Hysterectomy with salpingo-oophorectomy
0
68
p<0.000001*
p†
p<0.0001** p<0.0001**
†p<0.05 proves a statistically signi cant di erence between batches studied
* Fisher’s exact test
** Chi-square test
Analyzing the frequency of surgical interventions by
cases from the batch of patients treated by laparotomy
pathologies, we can observe that in the case of benign
(Table III; Figure 3).
ovarian tumors more numerous were cystectomies,
ere were registered statistically signi cant
followed by salpingo-oophorectomies, unilateral
di erences in the two batches also in the case of tubal
oophorectomies and salpingectomies,
without
pregnancy, where salpingectomy, prevailed in patients
statistically signi cant di erences, except for the
treated by laparotomy
(60 vs.
12).
is surgical
unilateral oophorectomy practices in a larger number of
indication was determined by the presence of the severe
48
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figure 5. Distribution of patients with adnexal torsion
Figure 6. Distribution of patients with benign tuboovarian
depending on the surgical procedure
pathology depending on the average of surgical
and postsurgical indices
Table IV. Results concerning indices of surgery, morbidity and hospitalization between the two batches
Group S
Group C
p†
n=636
n=602
Surgery time (min.)
90.81±18.12 (60-120)
81,16±23,46 (40-120)
p<0.0001*
Antiemetic postsurgical dosage (mg)
3.8±4.7
5.9±9.1
p<0.0001**
Postsurgical parenteral dosage of analgesic (mg)
10.5±21.8
149.8±81
p<0.0001**
Blood loss (ml)
78±41.80 (5-150)
157±84.59 (20-600)
p<0.0001*
e lowest percentage of oxygen saturation (%)
99.1±0.7
99.1±0.4
p=1.0000**
Postsurgical complications
37 (5.81%)
48 (7.97%)
p=0.144552***
Cystitis
28 (4.4%)
12 (1.99%)
p=0.023237***
Pelvic infections
0
12 (1.99%)
Surgical wound infection
8 (1.25%)
22 (3.65%)
p=0.020260***
Blood transfusion
1 (0.15%)
2 (0.33%)
p=1.000000***
Feverish morbidity
19 (3.1%)
139 (23.1%)
p<0.000001***
Postsurgical hospitalization period (days)
3.0±1.0
5.0±1.3
p<0.0001**
Postsurgical recovery period (weeks)
1.0±0.3
3.0±0.3
p<0.0001**
†p<0.05 proves a statistically signi cant di erence between the studied batches
* the Mann-Whitney test
** Comparison of means (t-test)
*** Fisher’s exact test
clinical background characterized by the presence of
treated by laparotomy, with a statistically signi cant
hemodynamic instability, the hemoperitoneum and the
di erence between the two batches (Table III; Figure 5).
size of the gestational sack of over 5 cm, which has led in
Analyzing the surgical indices we concluded that
many cases to the rupture of the Fallopian tube. In the
the surgery time was in average of 90.81 minutes for
batch of patients treated by laparoscopy, salpingectomy
laparoscopy, as compared to laparotomy where it was in
was performed under hemodynamic stable conditions
average of 81.16 minutes (p<0.0001). e intra-surgical
(Table III; Figure 4).
blood loss was signi cantly lower in the batch of patients
85.71% of the patients treated by laparoscopy for
treated by laparoscopy as compared to those treated by
adnexal torsion, considering the preservation of the
laparotomy (78±41.80 vs. 157±84.59; p<0.0001) (Table
ovarian function and implicitly of the fertile one, taking
IV; Figure 6). e lowest percentage of oxygen saturation
into account the young patients, the surgical detorsion
was of 99%, with no signi cant di erences between
associated with cystectomy was performed. e unilateral
batches.
adnexectomy was reserved for patients at menopause and
e postsurgical complications were more frequent
in cases where the sanguine ux and the normal color of
in the laparotomy group as compared to the study batch.
the ovary could not be restored after the surgical
ese were represented by cystitis, pelvic infections,
detorsion. is was performed predominantly in patients infections of the surgical wound and blood transfusions.
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
49
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
twenty.
e annual incidence of IPD in women aged
between 15-39 years seems to be of 10-13 cases in1000
women with a top incidence of around 20 cases in 1000
women 20-24 years old [5].
A real fact con rmed by statistic studies is that 75%
of IPD is caused by sexually transmitted diseases, 20% of
iatrogenic maneuvers while abortions and puerperal
infections have an incidence close to 5%. According to
the OMS 2008 estimations, 499 million of new cases of
curable infections with sexual transmission (e.g. syphilis,
gonorrhea, Chlamydia, trichomoniasis) happen annually
Figure 7. Distribution of patients with benign tuboovarian
all over the world, in adults aged between 15-49 years
pathology depending on the hospitalization/recovery period
[6]. IPD is most frequently observed in young women
and very rarely in women at post-menopause. Less than
ere were statistically signi cant di erences between
2% of the menopause women have IPD [7]. us, the
the two batches in the case of cystitis which prevailed in
risk factors for IPD include several sexual partners, a
the patients treated by laparoscopy, the pelvic infections
previous history of sexual transmitted diseases and a
and infections of the surgical wound which prevailed in
history of sexual abuse
[8]. Gynecological surgical
the patients treated by laparotomy
(p<0.05).
ree
procedures as the endometrium biopsy, curettage and
patients needed blood transfusions after a ruptured
hysteroscopy that penetrate the barrier of the cervix
ectopic pregnancy, one treated by laparoscopy and two
make women vulnerable to ascendant infections [9,10].
treated by laparotomy, this complication being without
Nonetheless, any woman with functional ovary may
statistic signi cance (Table IV).
experiment an ectopic pregnancy, starting with the age
Moreover, the postsurgical parenteral dosage of
of the menarche until menopause. Women of 40 years
analgesic and that of antiemetic were signi cantly
old proved to have a quota ratio adjusted by 2.9 of
smaller after laparoscopy, as compared to laparotomy
ectopic pregnancy.
[11]. A highest rate of ectopic
(p<0.0001) (Table IV).
pregnancy appears in women aged 35-44 years old One
Feverish morbidity de ned as fever
>38°C,
explanation is that aging may lead to a progressive loss
measured twice in 24 hour postsurgically, except for the
of the myoelectric activity in the fallopian tube,
rst 24 hours after the surgery, was found in 19 patients
responsible with the tubes’ motility [12].
treated by laparoscopy, as compared to 139 patients
Ovarian cysts, by far the most frequent condition as
treated by laparotomy (p<0.000001) (Table IV).
it may be seen also from our statistics (71.97%), are the
Prophylaxis with antibiotics was not used routinely,
prerogative of the “menstrual” period of the woman,
except for tubo-ovarian abscess.
e hospitalization
considering that in the mechanism of production the
indices show a period of postsurgical hospitalization and
hormonal changes play a determinant role.
a period of postsurgical recovery signi cantly shorter in
Predominance of this pathology in the extreme periods
the batch of patients treated by laparoscopy as compared
of genital life; puberty and pre-menopause when also
to the batch of patients treated by laparotomy
the
hypotalamo-hypophisis-ovarian
correlation
(p<0.0001)
(Table IV; Figure
7). After the clinical
disorders are more frequent.
e cysts of functional
reevaluation visit after 4 weeks since surgery, the patients
ovaries may appear at any age (inclusively in utero), but
went back to their normal routine.
they are much frequent in women of reproductive age.
ey rarely appear after menopause. Luteal cysts appear
Discussions
after ovulation in women of reproductive age.
e
majority of neoplasic benign cysts appear during the
Age, considered an epidemiologic factor, has a great
fertility years but the age interval is large and they can
importance in the tuboovarian pathology, some
appear at persons of any age [13].
conditions from this sphere being net predominant in
Related to the epidemiologic data from the specialty
some ages, being in uenced by hormonal changes and
literature and from our study the age average of patients
also by sexual habits.
with tuboovarian pathology was around 34-35 years
Annually, approximately 1 million women develop
with an age interval between
18-58 years, without
IPD [4]. It is estimated that around one of eight
statistically signi cant di erences between the two
adolescents sexually active develop BIP before they turn
studied batches.
50
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
e origination of patients from the rural or urban
benign ovarian tumors distribution correspond to those
environment is not an indicator to allow drawing
from the literature, having statistic signi cance (p<0.0001).
conclusions. e assignment of the cases does not attest
In consequence, the ectodermoid, dermatoid and
a statistically signi cant di erence between batches.
functional cysts represented more than a half (71.93%) of
Similar to the literature, the present study
the benign ovarian tumors pathology, followed by the
demonstrates that women at fertile age, with a sexually
serous cysts, mucinous cysts, hydropiosalpinx, simple
active life, are more exposed to the risk of benign tubo-
cysts, ovarian bromas and parovarian cysts.
ovarian pathology diseases, as compared to those in
Statistically there were no signi cant di erences
menopause. Parity did not register statistically signi cant
between batches concerning the tuboovarian pathology,
di erences between batches.
except for the mucinous, serous, parovarian cysts and
e use of an IUD was connected to a risk of 2 up
the adnexal torsion which predominated in the batch of
to
9 times higher for IPD and, implicitly for the
patients treated by laparoscopy.
tuboovarian abscess but the IUD used currently may
Considering the fertile age of casuistic the surgical
represent a substantially smaller risk
[14]. In a
interventions were conservatory.
e indications for
retrospective study of large cohort of 2012, the global
laparoscopy were the hemodynamic stability, the
risk of IPD in women which had IUD was of 0.54%
diameter of the benign tumor formation <10 cm and
[15]. Kelly and collaborators reported 9.6 cases of BIP
the wish to preserve fertility. Laparotomy was indicated
at 1000 IUD insertions, with the most signi cant risk
in cases with hemodynamic instability.
in the rst 20 days [16]. Meirik and collaborators have
In the total group of patient cystectomy prevailed in
validated the risk for IPD in the rst month after
(34.08%), followed by salpingo-oophorectomies,
insertion, this being connected to the number of sexual
arectomies, salpingectomies, unilateral oophorectomies,
partners, the age of the patient and the prevalence of
unilateral adnexectomies, hysterectomies with salpingo-
sexually transmitted diseases [17]. In our study as well
oophorectomies and salpingostomies, with statistically
the IUD bearer patients had an increased risk of the
signi cant di erence.
tuboovarian abscess occurrence, with a statistically
Comparing the two batches one may observe that
signi cant di erence between batches (p<0.05).
there are statistically signi cant di erences in the case of
e pathology of the tuboovarian region has proven
unilateral oophorectomy and salpingectomy, which
to be complex so the clinical background is also
prevailed in the patients treated by laparotomy.
extremely varied. If acute pelvic pain and the presence
Salpingotomy was performed only in patients
of a pelvic mass are symptoms and signs characteristic
treated by laparoscopy, where tubal pregnancy was
for a pelvic acute pathology, like a much voluminous
smaller than 5 cm, the gestation sack was localized in
ovarian cyst, a tuboovarian abscess, an ectopic pregnancy
the ampoule or the isthmic portion, the fertile function
or adnexal torsion, surely dysmenorrhea, menstrual
preservation was desired and the hemodynamic status
disorders, presence of pelvic adhesions and chronic
was stable.
pelvic pain were suggestive for the pelvic in ammatory
e hysterectomy with salpingo-oophorectomy was
disease, including pelvic endometriosis and everything
a purely laparotomic surgical intervention, practiced on
this disease implies. Acute pelvic pain was the main
patients with severe tuboovarian abscess, meaning an
symptom that dominated the clinical background in
ultrasound diameter bigger than 10 cm, with signs of
both batches, followed by the presence of a pelvic mass,
peritoneal irritation, septic state and instable
dysmenorrheal, menstrual disorders, the presence of
hemodynamic status.
mild-moderate pelvic at the laparoscopic diagnose
e rotation of adnexa around the vascular pedicle
examination and the chronic pelvic pain, with
may lead to total or partial occlusion of blood supply,
statistically signi cant di erences between variables.
leading to physical signs and symptoms compatible with
Lok and collaborators [18], in a study performed on
an acute abdomen that may progress to a potential
500 women operated laparoscopically for ovarian cystic
surgical emergency.
is has something in common
pathology, have found endometriomas
(44.5%) and
with the presence of cysts
[20]. Evaluation and
dermoid cysts (24.3%) representing more than two thirds
laparoscopic surgical treatment is indicated to prevent
of cases, followed by functional cysts
(6.6%).
e
the continuous damage of the ovary. Descargues et al.
pathological distribution in another large study had
have assessed
41 cases of ovarian torsions in which
included, in order of frequency, endometriomas, benign
caused pain, nausea and leukocytosis
[21].
irteen
adenomas, follicular cysts, corpus luteum cysts and
patients were treated by laparoscopy, out of which 11
dermoid tumors [19]. In our study also the results of
underwent a conservatory treatment by detorsion of the
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
51
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
adnexa and oophorectomy. None of these patients had
after laparoscopy as compared with laparotomy; the
surgical complications. Shalev and Peleg have managed
feverish morbidity was found in 19 patients treated by
41 patients with adnexal torsion by laparoscopic
laparoscopy, as compared to 139 patients treated by
detorsion reporting a postsurgical recovery free of events
laparotomy.
e period of postsurgical hospitalization
with restoring the ovarian function in 14 patients [22].
and the period of postsurgical recovery were signi cantly
Cohen et al. have evaluated 58 cases of ovarian torsion
shorter in the batch of patients treated by laparoscopy as
with adnexal ischemia met at laparoscopy and
compared to those treated by laparotomy.
conservatory managed by detorsion [23]. Oelsner and
In conclusion, the present study demonstrates the
al. have analyzed a total of 102 patients, 67 treated by
feasibility, safety and e cacy of the laparoscopic
laparoscopy and 35 by laparotomy, in order to determine
treatment as compared with the conventional laparotomy
if the ovary resumes its normal function after the simple
in the benign pathology of the tubo-ovarian region.
detorsion
[24].
93% of the patients treated by
laparoscopy presented full recovery of the follicular
function evaluated by transvaginal ultrasound, observing
References
signi cantly less intra-surgical complications in the
laparoscopic group as compared with the group treated
1.
Medeiros LR, Stein AT, Fachel J, Garry R, Furness S.
by laparotomy. Oelsner and al. have also reported in a
Laparoscopy versus laparotomy for benign ovarian
di erent study that 88-100% of the patients resume the
tumor: a systematic review and meta-analysis. Int J
ovarian function irrespective of the initial aspect of the
Gynecol Cancer 2008;18(3):387-99.
a ected ovary [25]. Our own study approaches the same
2.
Nezhat CR, Nezhat FR, Metzger DA, Luciano AA.
therapeutic attitude in a percentage of
85.71% in
Adhesion reformation after reproductive surgery by
patients treated by laparoscopy, taking into account the
videolaseroscopy. Fertil Steri 1990; 53(6):1008-11.
preservation of the ovarian function and, implicitly of
3.
Berek & Novak’s. Gynecology - 15th ed.,2012 by
the fertile function, considering the young patients. e
Lippincott Williams & Wilkins, a Wolters Kluwer
unilateral adnexectomy was reserved for patients at
business; pag. 1642.
menopause and in cases when the sanguine ux and the
4.
US National Library of Medicine, National Institutes
normal color of the ovary could not be restored after the
of Health. Pelvic in ammatory disease (PID). http://
surgical detorsion, being mostly practiced in patients
treated by laparotomy.
htm.
For the last twenty years, in comparison with
5.
Anjali Agrawal, MD. Imaging in Pelvic In ammatory
laparotomy, laparoscopy has constantly demonstrated
Disease and Tubo-Ovarian Abscess. Available at http://
decrease of intra-surgical blood loss, decrease of adhesions
emedicine.medscape.com/article/404537-overview.
formation, reduction of the hospitalization period, of
6.
Avan BI, Fatmi Z, Rashid S. Comparison of clinical
postsurgical pain and of the postsurgical recovery period,
and laparascopic features of infertile women su ering
allowing the patient to resume as quickly as possible their
from genital tuberculosis (TB) or pelvic in ammatory
normal routine [2,3]. e present study also demonstrates
disease
(PID) or endometriosis. J Pak Med Assoc
this fact: the surgery time was in average of 90.81 minutes
2001;51(11):393-9.
for laparoscopy and 81.16 minutes for laparotomy; the
7.
Heaton FC, Ledger WJ. Postmenopausal tuboovarian
loss of intra-surgical blood was signi cantly lower in the
abscess. Obstet Gynecol 1976;47(1):90-4.
batch of patients treated laparoscopically, comparative
8.
Champion JD, Piper J, Shain RN, Perdue ST,
with those treated by laparotomy; the postsurgical
Newton ER. Minority women with sexually transmitted
morbidity was present in proportion of 5.81% in patients
diseases: sexual abuse and risk for pelvic in ammatory
treated laparoscopically and 7.97% in those treated by
disease. Res Nurs Health 2001;24(1):38-43.
laparotomy; the patients treated laparoscopically
9.
Koumans EH, Kendrick JS. Preventing adverse
presented postsurgical cystitis and those treated by
sequelae of bacterial vaginosis: a public health program
laparotomy had postsurgical complications like infection
and research agenda. Sex Transm Dis 2001;28(5):292-
of the surgical wound and pelvic infections.
ree
7.
patients needed blood transfusions after a ruptured
10.
Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis
ectopic pregnancy, one treated laparoscopically and two
and risk of pelvic in ammatory disease. Obstet Gynecol
by laparotomy, this complication having no statistic
2004;104(4):761-9.
signi cance.
e parenteral postsurgical dosages of
11.
Bouyer J, Coste J, Shojaei T, et al. Risk factors for
analgesic and of antiemetic were signi cantly smaller
ectopic pregnancy: a comprehensive analysis based on a
52
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
large case-control, population-based study in France. Am
ovarian cyst. J Am Assoc Gynecol Laparosc 2000;7(4):
J Epidemiol 2003;157(3):185-94.
529-34.
12.
Vicken P Sepilian, Reproductive Endocrinology and
19.
Mettler L, Semm K Shiver K. Endoscopic management
Infertility, CHA Fertility Center. Ectopic Pregnancy.
of adnexal masses. JSLS 1997;1:103-12.
Available
at
20.
Nezhat CR, Kalyoncu S, Nezhat CH, Johnson E,
article/2041923-overview#aw2aab6b2b3aa
Berlanda N, Nezhat F. Laparoscopic management of
13.
C William Helm. Ovarian cyst. Available at http://
ovarian dermoid cyst: ten years’ experience. JSLS 1999;3
emedicine.medscape.com/article/255865-
(3):179-84.
overview#a0156
21.
Descargues G, Tinlot-Mauger F, gravier A, Lemoine
14.
Shelton JD. Risk of clinical pelvic in ammatory disease
JP, Marpeau L. Adnexal torsion: a report on forty- ve
attributable to an intrauterine device. Lancet
cases. Eur J Obtet gynecol Reprod Biol 2001;98(1):91-
2001;357(9254):443.
6.
15.
Workowski KA, Berman SM. Sexually transmitted
22.
Shalev E, Peleg D. Laparoscopic treatment of adnexal
diseases treatment guidelines, 2006. Centers for Disease
torsion. Surg Gynecol Obstet 1993;176(5):448-50.
Control and Prevention MMWR Recomm Rep.
23.
Cohen SB, Oelsner G, Seidman DS, Admon D,
2006;55(RR-11):1-94.
Mashiach S, Goldenberg M. Laparoscopic detorsion
16.
Kelly EK, Rudinsky SW. Intrauterine contraception:
allows sparing of the twisted ischemic adnexa. J Am
current evidence-based recommendations. J Midwifery
Assoc Gynecol Laparosc 1999;6(2):139-43.
Womens Health 2007;52(5):505-7.
24.
Oelsner G, Cohen SB, Soriano D, Admon D,
17.
Meirik O. Intrauterine devices
- upper and lower
Mashiach S, Carp H. Minimal surgery for the twisted
genital tract infections. Contraception
2007;75(6
ischaemic adnexa can preserve ovarian function. Hum
Suppl/):S41-7.
Reprod 2003;18(12):2599-602.
18.
Lok IH, Sahota DS, Rogers MS, Yuen PM.
25.
Oelsner G, Shashar D. Adnexal torsion. Clin Obstet
Complications of Laparoscopic surgery for benign
Gynecol 2006;49(3):459-63.
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
53
Photos from Medical Days of Satu Mare, 11th Edition
GENERAL REVIEW
ADOPTIVE CELL TRANSFER A NEW HOPE FOR METASTATIC
MELANOMA PATIENTS. A REVIEW
Golan Bubis1, Călin Bumbulu2, Lea Rath-Wolfson3
1Biology Faculty, the Hebrew University, Jerusalem, Israel,
2SCM dr Bumbulu -dr Balaj, Satu Mare, România,
3Department of Pathology, Hasharon Hospital, Petah-Tikva, a liated to Sackler School of medicine Tel-Aviv University,
Israel
Short title: Adoptive cell transfer, Metastatic melanoma
Address for correspondence:
Golan Bubis
Email: bubisgolan@gmail.com
Received: 15.07.2014
Accepted: 20.08.2014
Med Con October 2014, Vol 9, No 3, 55-58
Abstract
simpli ed this therapy may be o ered by growing
numbers of cancer institute’s.
One of the new treatments of metastatic melanoma
Keywords: metastatic melanoma, adoptive cell
is adoptive cell transfer (ACT) with autologous tumor
transfer, tumor in ltrating lymphocytes
in ltrating lymphocytes (TIL) which have the capacity
to kill the melanoma cells. e aim of the present report
Introduction
is to review, compare and summarize the clinical trials of
ACT for metastatic melanoma. is treatment was rst
Patients with metastatic melanoma have a mean
introduced in the NIH.
e protocols include
survival of less than one year [1]. Adoptive cell transfer
lymphodepleting regimen with or without total body
(ACT) uses tumor in ltrating lymphocytes
(TIL)
irradiation, prior to TIL infusion.
e TILs were
harvested from the patient’s tumor, which are then
extracted from the patient’s melanoma and then
expanded to large numbers and transferred by infusion
expanded to large numbers and re-infused into the
back to the patient. ese cells have the capacity to kill
patient, followed by low or high dose of interleukin-2
the melanoma cells. We conducted a systematic review
(IL-2). ACT with TILs has been shown to achieve
of trials and observational studies of the treatment of
objective response (OR) in about 50% and complete
metastatic melanoma by ACT, comparing the di erent
response (CR) in about 10% of patients. In recent years
protocols and the clinical results.
some simpli cations of the techniques allowed more
Adoptive Cell Transfer is a promising but labor
centers to adopt this treatment, including centers in
consuming technique. Metastatic melanoma tumors are
Israel, Denmark, Sweden and others.
resected, cut up into small 3-5 mm2 fragments and
Conclusion: ACT immunotherapy is nowadays
placed in culture plates with growth medium and high-
considered as one of the most promising strategies
dose (HD) IL-2. e TILs are initially expanded for 3-5
against metastatic melanoma. It has the potential to
weeks to at least 50×106 cells. e cells are then subjected
stabilize and even cure the disease. As the techniques are
to a rapid expansion protocol over two weeks by
Adoptive Cell Transfer - a New Hope for Metastatic Melanoma Patients. A Review
55
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
stimulating the T cells. e expanded TIL (now billions
and a long survival. However this approach is too toxic
of cells) are washed, pooled, and infused into the
and requires a stem cell back-up each time, precluding
patient.
is is followed by one or two cycles of HD
its widespread application.
IL-2 therapy or low dose IL-2 which supports the
Tumor reactive TIL used in these studies required
persistence of the infused TIL in vivo. Before TIL
an extended duration of multiple micro-cultures and an
transfer, the patient is treated with a preparative regimen
individualized assay to identify tumor recognition.
using cyclophosphamide (Cy) and udaribine (Flu) that
However, many patients were not ultimately eligible for
transiently depletes host lymphocytes, in other studies
treatment because their TIL failed the test for tumor
additional total body irradiation was used.
e ACT
recognition, or rapid disease progression occurred
studies for metastatic melanoma are summarized in
during TIL generation.
us, the complex TIL
Table I.
production process was simpli ed and shortened by
In 1988 Rosenberg et al. from the National Cancer
generating “young” TIL for therapy, and the batch-
Institute, NIH, Bethesda, Maryland [2] conducted a
speci c assay for tumor recognition was eliminated [5].
trial involving 20 patients treated with cyclophosphamid
Besser et al.
[6] at Sheba Medical Center Israel
followed 36 hours later by the infusion of TIL and high
recruited
27 patients with metastatic melanoma for
dose interleukin-2 (IL-2). Eleven patients experienced
treatment with short term cultured TIL. Young TIL
measurable regression of multiple metastases. In 2005
cultures were successfully established in twenty patients
Dudley et al.
[3], from the same cancer center,
(74%), which was higher than with the traditional
summarized the results of
35 patients with similar
protocol. Ten patients experienced objective clinical
results. In 2011 Rosenberg et al. [4] summarized the
response with 2 showing complete regression of the
results of
93 patients receiving di erent protocols of
tumor. In 2013 a larger cohort of patients was reported
lymphodepletion prior to TIL infusion, all patients
with similar statistical results [7].
received a lymphodepleting regimen consisting of
Rhadvanyi et al. [8] presented the MD Anderson
cyclophosphamide at
60 mg/kg/d for
2 days and
experience with ACT in metastatic melanoma.
e
udarabine at 25 mg/m2/d for 5 days. Two groups
success rate in achieving TIL expansion was about 62%
received in addition total body irradiation absorbed
regardless of the type of prior therapy before the tumor
dose of 2 Gy or 12 Gy respectively.
ese patients
harvest.
ey had 48.4% of objective clinical response
received following TIL infusion autologous puri ed
and 6.5% complete response.
cryopreserved CD34+ hematopoietic stem cells. ese
Pilon- omas et al. [9] reported the results from
patients had 20%-40% of complete response respectively
the Mo tt Cancer Center and Research Institute,
Table I. Overview of the ACT studies: protocols and results
Objective
Institute
No of
Complete
Author
Year
clinical
Protocol
State
patients
Response**
Response*
Rosenberg [2]
1988
NIH Maryland
20
11 (55%)
0
TIL, IL-2 HD
Dudley [3]
2005
NIH Maryland
35
18 (51%)
3 (8.6%) Young TIL, IL-2 HD
Besser [6]
2010
Sheba Medical Center Israel
20
10 (50%)
2 (10%) Young TIL, IL-2 HD
43
21 (48%)
5(12%)
TIL, IL-2 HD
TBI 2 Gy
25
13 (52%)
5 (20%)
Rosenberg [4]
2011
NIH Maryland
TIL, IL-2 HD
TBI 12 Gy
25
18 (72%)
10 (40%)
TIL, IL-2 HD
Radvanyi [8]
2012
M D Anderson Texas
31
15 (48.4%)
2 (6.5%)
TIL, IL-2 HD
Copenhagen University
Ellebaek [11]
2012
6
4 (66%)
2 (33%)
TIL, IL-2 Low dose
Denmark
Pilon- omas [9]
2012
Mo tt Florida
13
5 (38%)
2 (15%)
TIL, IL-2 HD
Ulenhag [10]
2012
Uppsala University Sweden
23
5 (22%)
1 (4%)
TIL, IL-2 Low dose
Besser [7]
2013
Sheba Medical Center Israel
49
23 (47%)
5 (10.6%) Young TIL, IL-2 HD
Abbreviations: TIL - Tumor In ltrating Lymphocytes, IL-2 - Interleukin-2, TBI - Total Body Irradiation, HD - High Dose
* Complete Response: Disappearance of all the metastases
** Objective clinical response: At least a 30% decrease in the sum of the metastases was noted
56
Bubis et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
Tampa, FL USA. Nineteen patients were enrolled with
References
13 patients (68%) successfully completing treatment.
An overall 38% response rate among treated patients
1.
Tarhini AA, Agarwala SS. Cutaneous melanoma:
was achieved.
available therapy for metastatic disease. Dermatol
er
Ullenhag et al.
[10] from the Department of
2006;19(1):19-25.
Oncology, Radiology and Radiation Science, Uppsala
2.
Rosenberg SA, Packard BS, Aebersold PM, et al. Use
University, Sweden showed that ultrasound-guided core
of tumor in ltrating lymphocytes and interleukin-2 in
needle biopsy is a safe and inexpensive approach to
the immunotherapy of patients with metastatic
obtain tumor tissue for TIL generation, especially in
melanoma. A preliminary report. N Engl J Med
instances where surgery is contraindicated. TILs were
1988/319(25):1676-80.
used for treatment in combination with daily low dose
3.
Dudley ME, Wunderlich JR, Yang JC, et al. Adoptive
s.c. IL-2.
eir response rate was somewhat lower than
cell transfer therapy following non-myeloablative but
other cancer centers but still encouraging.
lymphodepleting chemotherapy for the treatment of
Ellebaek et al. [11] from the Center for Cancer
patients with refractory metastatic melanoma. J Clin
Immune erapy, Hematology, Copenhagen University
Oncol 2005;23(10):2346-57.
Hospital, Denmark reported the results of 6 treated
4.
Rosenberg SA, Yang JC, Sherry RM, et al. Durable
patients with very good results. ey also used low-dose
complete responses in heavily pretreated patients with
IL-2 that signi cantly reduced the toxicity of therapy. A
metastatic
melanoma using T-cell
transfer
case of TIL treatment was also reported from the
immunotherapy. Clin Cancer Res 2011;17(13):4550-
Biomedical Research Center,
e First Hospital of
7.
Kunming, Kunming, People’s Republic of China [12].
5.
Dudley ME, Gross CA, Langhan MM, et al. CD8+
Joseph et al. [13] investigated the best conditions for
enriched
“young” tumor in ltrating lymphocytes can
successful TIL outgrowth.
e overall, initial TIL
mediate regression of metastatic melanoma. Clin Cancer
outgrowth was successful in 62% of patients, but for
Res 2010;16(24):6122-31.
patient’s ≤30 years of age it was 94%. Bio chemotherapy
6.
Besser MJ, Shapira-Frommer R, Treves AJ, et al.
within 0 to 60 days of tumor harvest negatively impacted
Clinical responses in a phase II study using adoptive
the initial TIL outgrowth with a success rate of only
transfer of short-term cultured tumor in ltration
16% (P<0.0001), a fact that should be considered when
lymphocytes in metastatic melanoma patients. Clin
ACT treatment is planned. A subcommittee on adoptive
Cancer Res 2010;16(9):2646-55.
cell therapy suggested an approach using centralized cell
7.
Besser MJ, Shapira-Frommer R, Itzhaki O, Treves AJ,
expansion facilities that will receive specimens and ship
Zippel DB, Levy D. Adoptive transfer of tumor-
expanded TIL infusion products to participating
in ltrating lymphocytes in patients with metastatic
centers, to ensure maximal yield and product
melanoma: intent-to-treat analysis and e cacy after
consistency. If successful, this approach will de nitively
failure to prior immunotherapies. Clin Cancer Res
answer the question of whether ACT can enter
2013;19(17):4792-800.
mainstream treatment for cancer [14].
8.
Radvanyi LG, Bernatchez C, Zhang M, et al. Speci c
ere are many ongoing clinical trials on the
lymphocyte subsets predict response to adoptive cell
treatment of melanoma by ACT. ey can be found in
therapy using expanded autologous tumor-in ltrating
ClinicalTrials.gov. Most of them are performed in the
lymphocytes in metastatic melanoma patients. Clin
USA but there are also ongoing trials in the United
Cancer Res 2012;18(24):6758-70.
Kingdom, Sweden, Switzerland, Israel and others. As it
9.
Pilon- omas S, Kuhn L, Ellwanger S, et al. E cacy
stands, however, there are no ACT protocols approved
of adoptive cell transfer of tumor-in ltrating lymphocytes
by the US FDA or other international regulatory
after lymphopenia induction for metastatic melanoma. J
agencies for use in cancer patients.
Immunother 2012;35(8):615-20.
Conclusions: ACT immunotherapy is nowadays
10.
Ullenhag GJ1, Sadeghi AM, Carlsson B, et al. Adoptive
considered as one of the most promising strategies
T-cell therapy for malignant melanoma patients with
against metastatic melanoma. It has the potential to
TILs obtained by ultrasound-guided needle biopsy.
stabilize and even cure the disease. As the techniques are
Cancer Immunol Immunother 2012;61(5):725-32.
simpli ed this therapy may be o ered by growing
11.
Ellebaek E, Iversen TZ, Junker N, et al. Adoptive cell
numbers of cancer institutes. Future will tell whether
therapy with autologous tumor in ltrating lymphocytes
ACT will progress from clinical trials to approved
and low-dose Interleukin-2 in metastatic melanoma
treatment.
patients. J Transl Med 2012;10:169.
Adoptive Cell Transfer - a New Hope for Metastatic Melanoma Patients. A Review
57
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
12. Su X, Zhang L, Wu S, Jin L, Ye J, Guan Z, Chen R.
14. Weber J, Atkins M, Hwu P, Radvanyi L, Sznol M,
Cascading adoptive cell therapy for metastatic melanoma.
Yee C. Immunotherapy Task Force of the NCI
Cancer Biother Radiopharm 2011;26(3):401-6.
Investigational Drug Steering Committee. White paper
13. Joseph RW, Peddareddigari VR, Liu P, et al. Impact of
on adoptive cell therapy for cancer with tumor-
clinical and pathologic features on tumor-in ltrating
in ltrating lymphocytes: a report of the CTEP
lymphocyte expansion from surgically excised melanoma
Subcommittee on adoptive cell therapy. Clin Cancer
metastases for adoptive T-cell therapy. Clin Cancer Res
Res 2011;17(7):1664-73.
2011;7(14):4882-91.
58
Bubis et al
GENERAL REVIEW
LAPAROSCOPIC TREATMENT IN RECTAL CANCER. WHERE ARE WE
IN 2014?
George Dejeu, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Marius S rlea, Codru a Macovei
Surgery Clinic of Pelican Hospital, Oradea, România
Address for correspondence:
Dejeu George
Pelican Hospital Oradea, Str. C. Coposu nr 2, cod 410469, Oradea, jud. Bihor, România
Email: dejeu.george@gmail.com
Received: 22.08.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 59-62
Abstract
available to patients.
e disease a ects approximately
39,000 patients a year in the United States [2].
e
e adoption of laparoscopic proctectomy for rectal
treatment of rectal cancer is a separate entity from colon
cancer has been slow, primarily because of the technical
cancer, although much of the available data concerns
di culty of the procedure. e wide surgeon-to-surgeon
both, and the issues concerning the use of minimally
variability in disease-free survival and local pelvic
invasive approaches overlap. Minimally invasive
recurrence after open proctectomy probably is due to
resection of rectal cancers has been shown to be feasible,
di erences in surgical technique.
ese di erences are
and patient selection depends on both tumor and
likely to be magni ed when the challenge of laparoscopy
patient speci c factors [3,4]. Resection of a rectal cancer
is added to the procedure. Oncologic and functional
involves consideration of the tumor stage, level of the
outcomes data are limited. Although the adoption of
tumor within the rectum, mesorectal involvement, and
laparoscopic techniques to perform curative proctectomy
local invasion of adjacent organs [5].
likely will expand as technical challenges are overcome
e most important factor for any rectal cancer
and experience and training improve, the results of
operation should obviously be oncologic outcome. e
prospective multicenter trials are necessary to ensure
standard of care should be based on long-term survival.
that the procedures provide equivalent oncologic and
Obtaining this data, however, requires lengthy and
functional outcome to conventional surgery.
costly follow-up. Part of achieving a good oncologic
Rectal cancer remains a common and complex
outcome for rectal cancer is adherence to the principles
surgical problem.
ere is growing evidence that
of total mesorectal excision (TME) [6-8]. is has been
minimally invasive surgery (MIS) can provide ideal care
clearly established in the literature to lead to better
for patients with rectal cancer. Lap rectal cancer surgery
oncologic outcomes [9,10].
is the highest hill to climb in MIS cancer surgery [1].
Why is rectal cancer laparoscopic treatment such a
Keywords: laparoscopy, rectal cancer, proctectomy
di cult endeavor?
e anatomy of the rectum!
e
rectum is a thick tubular organ con ned in the narrow
Rectal cancer remains a challenging disease to treat,
bony pelvis. e operator has a view from above of what
but with the advent of MIS many new options are
can be compared to looking down a funnel that is
Laparoscopic Treatment in Rectal Cancer. Where Are We in 2014?
59
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
occupied almost entirely of the rectum.
is makes it
the technique still is not widely used.
e LRR
di cult to dissect, although the dissection plane, ‘the
procedure is technically demanding.
e signi cant
holy plane’ [10], is avascular, and easy to nd. e small
learning curve, the narrow con nes of the bony pelvis,
con nements of the pelvis, especially the male pelvis,
and the angling limits in current stapling technology,
make it di cult to section the rectum below the tumor,
together with the standard practice of autonomic nerve-
and the lower the tumor, the more di cult it gets to put
sparing total mesorectal excision (TME), have made
the stapler in a good position. All this must take into
laparoscopic surgery for rectal cancer more challenging
consideration the oncologic safety, that is the
[28]. Body habitus, local invasion, and other reasons
circumferential and distal margins.
e distal margins
may identify patients as unsuitable for LRR, and
that make the operation oncologicaly safe have gone
conversion rates tend to be higher than for colon cancer.
down over time, with only about 1cm being su cient in
SAGES at its consensus of laproscopic rectal cancer
the latest guidelines [11]. More important being the
surgery in 2006 says:
completion of surgery with tumor free circumferential
”Recommendation: Laparoscopic resection for rectal
resection margins (CRM). is means dissecting outside
cancer should follow standard oncologic principles:
what oma Ionescu rst named the ‘fascia propria’ of
adequate distal margin, ligation of the base of the superior
the rectum in 1894, and what we now call the mesorectal
rectal/inferior mesenteric artery, and mesorectal excision
fascia.
(Level II evidence, Grade B recommendation)
e word mesorectum was possibly rst used by
A distal margin of 1-2cm.
Maunsell in 1892 and was later popularized by Heald
Removal of the blood supply and lymphatics up to the
when re ering to what now is the ‘golden standard’ in
origin of the superior rectal artery (or inferior mesenteric
rectal cancer surgery, the Total Mesorectal Excision [6].
artery if indicated), and total mesorectal excision with
e mesorectum is composed of all the fat and lymphatic
radial clearance.
nodes that are enclosed within the mesorectal fascia (the
Recommendation: Adequate training and experience
‘fascia propria’ of the rectum) down to the pubo-rectalis
are necessary to perform an appropriate oncologic resection.
muscle. Total Mesorectal Excision implies the complete
(Level II, Grade B)” [11]
dissection and excision, en bloc with the tumor, the
European Association for Endoscopic Surgery and
rectum and the limpho-vascular supply, of all the fat
other interventional techniques (EAES) at its consensus
and lymph nodes enclosed int the mesorectal fascia, the
on rectal cancer laparoscopic treatment in 2010 says:
mesorectum down to the elevator muscles.
“As in open surgery, oncological principles (resection
Can it be done laparoscopically? It is di cult but it
margins, high vessels ligation, lymphadenectomy etc.)
can be done, and in fact it is done successfully around
should be respected by the laparoscopic approach. (92.9%
the world. Laparoscopy used for colorectal surgery has
[Consensus]; Grade of recomandation
(GoR)B: 92.9%
been gaining wider acceptance during the last decade.
[Consensus])
Several advantages of laparoscopic colorectal surgery are
e main goal is a tumor-free margin. Whenever
proven, including less postoperative pain, a shorter
possible a free margin should be obtained.
(92.9%
postoperative ileus, a shorter hospital stay, better
[Consensus]; GoRB: 85.7% [Consensus])
cosmetic, and favorable e ects on cytokine and
Pelvic dissection and rectal mobilization must be
hormonal responses
[12].
e landmark Clinical
performed according to TME principles. (100% [Strong
Outcomes of Surgical erapy (COST) Trial expanded
consensus]; GoRA: 92.1% [Consensus])
the laparoscopic trend to colon cancer, speci cally, with
EAES Consensus on rectal cancer laparoscopic
reports of oncologic equivalencies between the open and
treatment 2010
laparoscopic approaches and a bene t in terms of
Laparoscopic approach to TME is not inferior to the
secondary end points for the laparoscopic group [13].
open in terms of disease-free survival
(DFS), overall
More experience with laparoscopic rectal resection
survival
(OS) or local recurrence. (92.9% [Consensus];
(LRR) suggests that early oncologic outcomes are
GoR B: 85.7% [Consensus])” [29].
equivalent to those for open surgery
[12,14-21].
What about the robot?
Support for laparoscopic rectal resection in the treatment
e use of minimally invasive technology has had a
of primary rectal cancer has been described in a number
signi cant impact on colorectal surgery and every year
of reports [22,23], randomized trials [18,19,24,25] and
brings new applications [30]. Laparoscopic surgery does
meta-analyses [14,26,27].
have limitations, however.
e instruments are rigid,
Although the safety and oncologic equivalence of
restricting the surgeon’s movements, and this can be a
LRR and open surgery have been generally accepted,
signi cant disadvantage when operating in the narrow
60
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
con nes of the pelvis. Additionally, the surgical assistant
References
must have considerable experience to provide a stable
camera view and steady retraction. ese issues result in
1.
Marks J. Laparosopic surgery in rectal cancer, can it be
a steep learning curve; one study estimated that true
done? SAGES 2013, Colorectal MIS Postgraduate
pro ciency is achieved only after 50 cases [31].
Course, Baltimore MA.
Since the early 2000s, the use of a robotic surgical
2.
Jemal A, Siegel R, Xu J, Ward E. Cancer statistics,
platform has become increasingly popular. Robotic
2010. CA Cancer J Clin 2010;60(5):277-300.
technology may help overcome some of the limitations
3.
Leroy J, Jamali F, Forbes L, et al. Laparoscopic total
of laparoscopic colo- rectal surgery
[32]. Robotic
mesorectal excision
(TME) for rectal cancer surgery:
surgical instruments are exible and maneuverable,
long-term outcomes. Surg Endosc 2004;18(2):281-9.
providing wristed movement. is allows the surgeon to
4.
Lujan J, Valero Q, Hernandez A, et al. Randomized
reach around anatomic structures, to operate in small
clinical trial comparing laparoscopic and open surgery in
spaces, and to perform precise lateral dissection.
e
patients with rectal cancer. Br J Surg 2009;96(9):982-
robotic camera provides a high-de nition three-
9.
dimensional (3D) view; mounted on a robotic arm, it is
5.
Bleday R, Brindzei N. Surgical treatment of rectal
stable and con- trolled by the operating surgeon.
cancer.
e ASCRS textbook of colon and rectal
Lastly, it has been estimated that the learning curve
surgery, 2011;731-41.
is reached after approximately
20 cases, even for
6.
Heald RJ, Husband EM, Ryall RD. e mesorectum
surgeons who lack signi cant laparoscopic experience
in rectal cancer surgery-the clue to pelvic recurrence? Br J
[33]. Because the robot a ords improved visualization
Surg 1982;69(10):613-6.
and manipulation, facilitating precise dissection within
7.
MacFarlane JK, Ryall RD, Heald RJ. Mesorectal
the con nes of the bony pelvis, the use of robotic-
excision for rectal cancer. Lancet 1993;341(8843):457-
assisted resection for patients with rectal cancer has been
60.
increasing.
8.
Quirke P. Training and quality assurance for rectal
e role of robotics in colorectal cancer surgery is
cancer:
20 years of data is enough. Lancet Oncol
still being de ned. Robotic technology shows great
2003;4(11):695-702.
promise, and studies to date have demonstrated its safety.
9.
Quirke P, Durdey P, Dixon MF, et al. Local recurrence
Some studies have shown that robotic colorectal cancer
of rectal adenocarcinoma due to inadequate surgical
surgery is clearly superior to laparoscopy in reducing
resection. Histopathological study of lateral tumor spread
rates of intraoperative conversion, a nding that is most
and surgical excision. Lancet 1986;2(8514):996-9.
likely the result of better optics, instrumentation, and
10.
Heald RJ, Moran BJ, Ryall RD, et al. Rectal cancer:
retraction. Whether robotic surgery for colorectal cancer
the Basingstoke experience of total mesorectal excision.
will improve long-term outcomes, such as sexual and
Arch Surg 1998;133(8):894-9.
urinary function, remains unclear. As the use of robotic
11.
surgery grows, critical evaluation of results and outcomes
guidelines-for-laparoscopic-resection-of-curable-
is vitally important - not only to prevent undue harm to
colon-and-rectal-cancer/ accessed on
22/08/2014
patients but also to control the considerable nancial
15:20 GMT
challenges posed by this expensive new technology in
12.
Leung KL, Lai PB, Ho RL, et al. Systemic cytokine
our era of rising health-care costs. Additional high-
response after laparoscopic-assisted resection of recto
quality, randomized studies are needed to determine the
sigmoid carcinoma: a prospective randomized trial. Ann
real advantages and shortcomings of minimally invasive
Surg 2000;231(4):506-11.
robotic surgery for colorectal cancer.
13.
Clinical Outcomes of Surgical erapy Study Group.
MIS for rectal cancer has potential. Early data
A comparison of laparoscopically assisted and open
suggest improved short-term outcomes and no
colectomy for colon cancer. N Engl J Med
detriment to oncologic outcomes. Multi-institutional,
2004;350(20):2050-9.
randomized, controlled trials are underway. Education
14.
Anderson C, Uman G, Pigazzi A. Oncologic outcomes
and credentialing of surgeons in the MIS techniques for
of laparoscopic surgery for rectal cancer: a systematic
treatment of rectal cancer should ensure adoption of
review and meta-analysis of the literature. Eur J Surg
proper oncologic technique and result in appropriate
Oncol 2008;34(10):1135-42.
oncologic outcomes, assuming data are forthcoming
15.
Aziz O, Constantinides V, Tekkis PP, et al. Laparoscopic
that con rms MIS as an appropriate method to treat
versus open surgery for rectal cancer: a meta-analysis.
rectal cancer.
Ann Surg Oncol 2006;13:413(3)-24.
Laparoscopic Treatment in Rectal Cancer. Where Are We in 2014?
61
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
16.
Gao F, Cao YF, Chen LS. Meta-analysis of short-term
25.
Ng SS, Leung KL, Lee JF, Yiu RY, Li JC, Hon SS.
outcomes after laparoscopic resection for rectal cancer.
Long- term morbidity and oncologic outcomes of
Int J Colorectal Dis 2006;21(7):652-6.
laparoscopic-assisted anterior resection for upper rectal
17.
Lelong B, Bege T, Esterni B, et al. Short-term outcome
cancer: ten-year results of a prospective, randomized
after laparoscopic or open restorative mesorectal excision
trial. Dis Colon Rectum 2009;52(4):558-66.
for rectal cancer: a comparative cohort study. Dis Colon
26.
Huang MJ, Liang JL, Wang H, Kang L, Deng YH,
Rectum 2007;50(2):176-83.
Wang JP. Laparoscopic-assisted versus open surgery for rectal
18.
Lujan J, Valero G, Hernandez Q, Sanchez A, Frutos
cancer: a meta-analysis of randomized controlled trials on
MD, Parrilla P. Randomized clinical trial comparing
oncologic adequacy of resection and long-term oncologic
laparoscopic and open surgery in patients with rectal
outcomes. Int J Colorectal Dis 2011;26(4):415-21.
cancer. Br J Surg 2009;96(9):982-9.
27.
Ohtani H, Tamamori Y, Azuma T, et al. A meta-
19.
Ng SS, Leung KL, Lee JF, Yiu RY, Li JC, Teoh AY,
analysis of the short- and long- term results of randomized
Leung WW. Laparoscopic-assisted versus open
controlled trials that compared laparoscopy-assisted and
abdominoperineal resection for low rectal cancer: a
conventional open surgery for rectal cancer. J
prospective randomized trial. Ann Surg Oncol
Gastrointest Surg 2011;15(8):1375-85.
2008;15(9):2418-25.
28.
Row D, Weiser MR. An update on laparoscopic
20.
Staudacher C, Vignali A, Saverio DP, Elena O,
resection
for
rectal
cancer. Cancer Control
Andrea T. Laparoscopic vs open total mesorectal excision
2010;17(1):16-24.
in unselected patients with rectal cancer: impact on early
29.
Siegel R, Cuesta MA, Targarona E, et al. Laparoscopic
outcome. Dis Colon Rectum 2007;50(9):1324-31.
extra peritoneal rectal cancer surgery: the clinical practice
21.
Strohlein MA, Grutzner KU, Jauch KW, Heiss MM.
guidelines of the European Association for Endoscopic
Comparison of laparoscopic vs open access surgery in
Surgery (EAES). Surg Endosc 2011;25(8):2423-40.
patients with rectal cancer: a prospective analysis. Dis
30.
Peterson CY, Weise M R. Robotic Colorectal Surgery. J
Colon Rectum 2008;51(4):385-91.
Gastrointest Surg 2014;18(2):398-403.
22.
Baik SH, Gincherman M, Mutch MG, Birnbaum
31.
Li JC, Lo AW, Hon SS, Ng SS, Lee JF, Leung KL.
EH, Fleshman JW. Laparoscopic vs open resection for
Institution learning curve of laparoscopic colectomy-a
patients with rectal cancer: comparison of perioperative
multi-dimensional analysis. Int J Colorectal Dis
outcomes and long-term survival. Dis Colon Rectum
2012;27(4):527-33.
2011;54(1):6-14.
32.
Peterson CY, McLemore EC, Horgan S, Talamini
23.
Laurent C, Leblanc F, Gineste C, Saric J, Rullier E.
MA, Ramamoorthy SL. Technical aspects of robotic
Laparoscopic approach in surgical treatment of rectal
proctectomy. Surg Laparosc Endosc Percutan Tech
cancer. Br J Surg 2007;94(12):1555-61.
2012;22(3):189-93.
24.
Kang SB, Park JW, Jeong SY, et al. Open versus
33.
Jiménez-Rodríguez RM, Díaz-Pavón JM, de la
laparoscopic surgery for mid or low rectal cancer after
Portilla de Juan F, Prendes-Sillero E, Dussort HC,
neoadjuvant chemo radiotherapy
(COREAN trial):
Padillo J. Learning curve for robotic-assisted laparoscopic
short-term outcomes of an open-label randomised
rectal cancer surgery. Int J Colorectal Dis
controlled trial. Lancet Oncol 2010;11(7):637-45.
2013;28(6):815-21.
62
Dejeu et al
GENERAL REVIEW
MYOCARDIAL FIBROSIS A PATHOPHYSIOLOGICAL PROCESS IN
CARDIAC REMODELING
Lala I. Radu, Maria Puşchi ă
Faculty of Medicine, Pharmacy and Dentistry, West University “Vasile Goldis”, Arad, Romania
Address for correspondence:
Radu Lala, Maria Puschi ă
Faculty of Medicine, Pharmacy and Dentistry, West University “Vasile Goldis” Arad
86 Liviu Rebreanu St.
Email: radu_lala@yahoo.com, mpuschita@yahoo.com
Received: 05.09.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 63-68
Abstract
changes produced by myocardial damage, neurohormonal
activation and hemodynamic load. ese mechanisms
Heart failure is a clinical syndrome characterized by
will contribute in changing the structure and size of the
lack of pump due to reorganization of the underlying
heart with externalization in the end of speci c
normal cardiac structures, a process which is known as
symptoms. e myocytes is the main cell involved in this
„remodeling”. Heart failure is the leading cause of
process in addition to the interstitium and coronary
hospitalization in the elderly and is associated with
vasculature. Cardiac remodeling involves ischemic,
increased morbidity and mortality. e increased mortality
in ammatory,
brosis,
necrosis and apoptosis
in heart failure is mainly due to malignant arrhythmias
mechanisms [1].
and sudden death which are attributed to myocardial
Both neuro humoral and adrenergic activation are
brosis. Although not fully known all the mechanisms
increased in patients with heart failure, which
involved in ventricular remodeling, lately there has been
contributes signi cantly to the prognosis of the disease.
focus and intensive studies on myocardial brosis, a
Angiotensin II is one of the main mediators of cardiac
process underlying cardiac remodeling. Fibrosis is of
remodeling and its local production is mediated by the
multifactorial etiology, such as: ischemia, in ammation,
elongation of myocardial bers.
is peptide has a
hypoxia, vasoactive peptides, all of these mechanisms
proliferative and growth e ect on broblasts and
beeing responsible for development of heart failure.
myocytes that is manifested by DNA and protein
Keywords: remodeling, broblasts, brosis
synthesis. Angiotensin II also shows a cytotoxic e ect on
myocardial cells by activating the rennin angiotensin
The concept of cardiac remodeling in
aldosterone system which is exaggerated in heart failure
heart failure
[2-3]. An alternative way to the generation of
angiotensin II in the myocardium is chymase pathway
Cardiac
remodeling
is
a
determinant
which has higher speci city in converting angiotensin I
pathophysiological process of clinical outcome in heart
to angiotensin II. Chymases are stored in the cytoplasmic
failure based on molecular, cellular and interstitial
granules of mast cells whose density increases in heart
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
63
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
failure.
e cymase pathway is important in promoting
phenotype (secretory, proliferative, and migratory) is
brosis in heart failure and its inhibition may represent
performed by neurohormonal activation and mechanical
a potential therapy in regression of cardiac remodeling
stress [10]. Predominant action of angiotensin II takes
[4]. Myocytes elongation due to myocardial damage will
place on AT1 receptors which are expressed by
increase local activity of norepinephrine, angiotensin
myo broblasts this leading in to synthesis of collagen I,
and endothelin, which in turn will lead to myocytes
III and bronectin
[11]. Endothelin-1 acts on the
hypertrophy, collagen synthesis with matrix formation
myo broblasts ETA and ETB receptors that will result
that will end up with myocardial brosis
[1]. To
in increased synthesis of collagen and reduced collagenase
compensate for heart pump de ciency after myocardial
activity [12]. Catecholamines determine the modulation
insult, catecholamine will act directly on cardiomyocytes
of cardiac broblasts by stimulating secretion of cytokines
exerting chronotropic and inotropic e ects. Also they
and growth factors
[9]. Mechanical stress activates
have a cytotoxic e ect by promoting subendocardial
broblasts via integrin, secondary ion channel or cellular
myocytes necrosis [5].
signaling, leading to increased secretion of matrix
e main components of cardiac remodeling are:
proteins, growth factors and metalloproteinases [10].
the myocytes, broblast proliferation, apoptosis and
Myo broblasts are cells with proliferating,
degradation of collagen. During remodeling cardiac
migratory and secretory properties and express
myocytes begin to decrease in number due to cardiac
contractile proteins such as alpha-SMA (smooth muscle
insult, the remaining ones will be part of the
actin). Myo broblasts are responsible for the secretion
compensatory mechanism involving elongation or
of in ammatory mediators such as cytokines
(TNF
hypertrophy to maintain cardiac output under normal
alpha, TNF, IL-1, IL-6, TGF-beta), vasoactive peptides
conditions [1]. Impaired ventricular lling will determine
(angiotensin II, endothelin-1, atrial natriuretic factors
contractile protein synthesis in myocytes that will induce
ANP and BNP), and hormones (norepinephrine) whose
new sarcomere organization which will establish either
serum concentration is increased in cardiac remodeling.
elongation or cell hypertrophy, but everything at the cost
eir function is altered by the action of stimuli like:
of oxygen and energy consumption. is will create a
myocytes elongation, myocardial ischemia and
vicious circle that will lead to myocardial ischemia and
reperfusion. As a consequence of their altered function
myocardial cell loss
[6]. In response to myocardial
the extracellular matrix turn-over will su er changes
ischemia broblast proliferation will stimulate collagen
through the increased secretion of metalloproteinases
synthesis that will lead up to patchy ventricular brosis
(enzymes degrading collagen) and in ammatory
and thus contributing to remodeling [7].
mediators, that regulate TIMP
(tissue inhibitors of
metalloproteinases) [9].
The role of fibroblasts in cardiac
Phenotypic transformation of broblasts into
remodeling
myo broblasts is not found in the normal myocardium,
however their number abound in the surrounding areas
Fibroblasts are the main cells responsible for the
of myocardial infarction where the synthesis and
secretion of excess extracellular
matrix and
deposition of collagen forms up the brotic scar tissue
cardiomyocytes hypertrophy via paracrine mechanisms
[13]. Once the maturation of the scar done, the
in cardiac remodeling, all of which contribute to
myo broblasts will undergo an apoptosis with the
decreased myocardial contractile function [8]. Fibroblasts
remanence at this level of acellular components (collagen
represent 70% of cardiac cells having the main function
matrix proteins). However, repeated injury of the
to secrete extracellular matrix proteins that provide
myocardium will counterbalance apoptotic process with
compact structure of the heart and transmission of
persistence of myo broblasts in the scar tissue [14].
mechanical, chemical and electrical signals between
Basically, further persistence of myo broblasts directly
cellular and a cellular component of the heart. e most
facilitates myocardial brosis leading up to pathological
important protein components of the extracellular
remodeling and progression to heart failure. In
matrix are collagen that forms a network around
experimental models on mice, was observed persistence
myocytes, tolerant to mechanical stress [9]. Fibroblasts
of myo broblasts in the healing area months after the
play a key role in the pathology of cardiac remodeling in
infarction [15].
e post-mortem studies in humans
hypertension and myocardial infarction [9].
observed the presence of these cells in the myocardium
Negative e ects on the heart are expressed by
for months or years [16].
broblasts by their di erentiation into myo broblasts.
Fibroblasts are more than mere collagen-forming
Activation of broblast with acquisition of a transitory
cells; they have been termed sentinel cells with local
64
Radu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
immunomodulatory function [17]. Fibroblasts have the
ere have been described two forms of myocardial
following function: extracellular matrix homeostasis, the
brosis: reactive interstitial
brosis reactive and
production of bioactive molecules, heart blood vessels and
substitutional brosis.
e rst variant was observed in
cardiac electrophysiology homeostasis
[8]. All these
ventricular overload (hypertension, aortic stenosis) as an
features are manifested in response to changes that occur
adaptive response to increased pressure exerted at this
in their environment to preserve the proper functioning
level which evolves initially without loss of
of the heart. Homeostasis is shown by the secretion of the
cardiomyocytes. If the obstacle generating increased
extracellular matrix of brillar collagen type I and III, the
pressure in the left ventricle is not eliminated, reactive
most abundant myocardial collagen and collagen type IV,
brosis will nally progress to substitutional brosis
V, VI, elastin, and laminin less abundant, all in response
characterized by cardiomyocytes hypertrophy and
to the action of growth factors, cytokines or mechanical
necrosis [26].
e second form, meaning substitutional
stimulation [18]. rough secretion of bioactive molecules
brosis is seen in myocardial infarction as an immediate
cell proliferation, apoptosis and contractions are
process consecutive to myocardial in ammation and
controlled. Fibroblasts may induce angiogenesis by
cell death [27]. In the initial phase of cardiac remodeling
secretion of vascular growth factors (VEGF, FGF) from
broblasts undergo apoptosis but later this compensatory
pre-existing vessels, a phenomenon that was also observed
mechanism will be overcomed by persistent formation
in preconditioned ischemia
[19]. Fibroblasts also
of extracellular collagen in response to myocardial injury
contribute to normal cardiac electrophysiology by forming
with nal progression to heart failure [8].
e harmful
a layer of extracellular matrix that separates electrical
e ects of excessive synthesis of extracellular matrix on
activity of certain myocytes groups.
is phenomenon
the heart pump function manifest itself in several ways.
was seen in the valvular brous ring that separates the
On one hand there is an increase in mechanical sti ness
electrical activity of the atria from the ventricles [20]. It
with diastolic dysfunction, on the other hand the
has been shown that broblasts can be coupled to
arrangement of collagen through cardiomyocytes will
myocytes through connexins that may result in activation
disrupt intercellular electrical coupling leading to
of separated myocytes groups with formation of reentry
impaired systolic function [28]. Also, in ammation and
circuits and cardiomyocytes synchronization activity [21-
coronary perivascular brosis will reduce locally the
22]. Approximately
30% of the activated cardiac
ow of oxygen and nutrients, which will lead to
broblasts originate from endothelial cells that undergo a
augmentation of cardiac remodeling
[29]. Fibrotic
process known as endothelial mesenchymal transition
remodeling involves the associated action of
(TME) [23]. Endothelial cells under the action of stimuli
metalloproteinases and humoral factors (angiotensin II,
such as hypoxia or TGF-beta will acquire a broblast-like
endothelin-1, TGF-beta, TNF-alpha) which happen to
phenotype with loss of characteristic endothelial features.
be in increased number [10]. Metalloproteinases are
ese transitional cells contribute to myocardial brosis
considered to be major determinants of extracellular
through broblast proliferation with collagen synthesis
matrix remodeling post-myocardial infarction [30]. In
and micro vascular rarefaction [24]. Monocytes were set
rst phase the latter, by their
brillar collagen
as a potential source by the fact that in the infarcted tissue
degradation function will interrupt the interstitial
they were found to express the monocyte-speci c surface
matrix with increased in ammatory response that will
antigen, namely (CD45, CD11b) [25].
trigger broblast proliferation and di erentiation [10].
Electro physiologically, myocardial brosis impeds
Myocardial fibrosis in heart failure -
normal spread of excitation by creating an anisotropic
essential link
environment,
predisposing
to
increased
arrhythmogenesis
(blocks, reentry) a phenomenon
Most heart disease leading to heart failure is
frequently met in hypertrophy or myocardial ischemia
associated with the development of myocardial brosis.
[31]. Fibrosis can cause atrial or ventricular brillation
Myocardial brosis is the scarring of the myocardium
by modulating the formation of early post potentials
through the accumulation of broblasts, and the
leading to trigger activity [32-33]. Myocardial brosis
secretion of excess extracellular matrix that will lead
not only determines arrhythmias through a reentrant
them to change the structure and the organic architecture
mechanism but also by trigger activity through an
of the heart [8]. Excessive accumulation of extracellular
abnormal growth in automaticity [34].
matrix will increase heart sti ness with induction of
Myocardial
brosis is considered a major
pathological signs at myocytes level and progression to
determinant of diastolic dysfunction and impaired
heart failure [8].
pump function of the heart in hypertensive patients
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
65
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
[35]. Querejeta et al.
[35,36] in their studies have
extracellular matrix low in collagen. All of these result in
demonstrated an association between myocardial
scar formation but with free-standing connective tissue
accumulation of collagen type I bers and deterioration
[42].
e immediate consequence is cardiac remodeling
of cardiac function in hypertensive patients by
with ventricular dilatation and severe systolic dysfunction,
measurement of serum carboxy-terminal pro-peptide of
which increases heart failure mortality and occurrence of
type I procollagen. Myocardial hypertrophy subsequent
mechanical complications such as myocardial rupture in
of hypertension is based on two important
the elderly.
pathophysiological mechanisms: myocytes hypertrophy
Cardiac and arterial brosis is common in patients
and progressive accumulation of interstitial brous
with diabetes and predisposes to heart failure. In large
tissue [35-37]. Myocardial brosis predisposes to heart
part this is due extracellular matrix remodeling through
failure, i.e. a 2, 3 times increase in the volume fraction
processes like ischemia, in ammation, oxidative stress
of collagen leads to diastolic dysfunction with
plus glycosylation end-products (AGE) that will a ect
preservation of systolic function, however, a further
the turnover of collagen [43].
increase in the volume fraction will alter the latter [38].
Sughira et al. and Oshato et al. showed a signi cant
Conclusions
association between collagen volume fraction and
diastolic dysfunction determination by echo Doppler in
Cardiac remodeling undoubtedly has a great clinical
hypertensive patients [38].
relevance
and
understanding
its
complex
In the elderly collagen deposition occurs in the
pathophysiological mechanisms is essential in nding
vascular wall, perivascular, myocardial interstitium and
therapeutic targets to halt this phenomenon with
this will have an impact by reducing myocardial and
potentially fatal clinical events. Myocardial brosis is an
vascular compliance [39].
us brosis in the elderly
important link in cardiac remodeling and behind this
will increase myocardial
sti ness with diastolic
mechanism lays the broblast cells with their numerous
dysfunction appearance. Interstitial brosis results from
functions that shape the heart architecture. Fully
collagen deposition at the level of peri- and endomysium
understanding their functioning remains an enigma to
while perivascular
brosis results from collagen
researchers; of other approach involves the discovery of
deposition at the adventiceal level of the intramural
new broblast markers.
coronary arteries [40]. Myocardial hypertrophy observed
in the elderly is a consequence of increased peripheral
Con ict of interest: Co- nancing: European Social
vascular sti ness that will entail hemodynamic load and
Fund Operational Programme Human Resources
in turn will lead to increased interstitial collagen
Development 2007-2013. (POSDRU/159/1.5/141531).
synthesis
[41]. Unlike in the hypertensive model in
e co-author reports no nancial support with commercial
which collagen synthesis is greatly increased, in the
interests.
elderly, brosis is primarily a consequence due to
reduced activity of metalloproteinases that are inhibited
by tissue inhibitors of metalloproteinases
(TIMP)
References
through the stimulatory action of TGF-beta [40]. In
practical terms it is a reduction in matrix degradation.
1. Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling--
Although diastolic dysfunction plays the main role in
concepts and clinicalimplications: a consensus paper
the pathogenesis of heart failure in the elderly, however,
from an international forum on cardiac remodeling.
brotic remodeling can a ect also systolic function by
Behalf of an International Forum on Cardiac
associated co morbidities like hypertension, diabetes or
Remodeling. J Am Coll Cardiol 2000;35(3):569-82.
coronary heart disease.
2. Sadoshima J, Izumo S. Molecular characterization of
Senescence hearts as opposed to the healthy ones
angiotensin II-induced hypertrophy of cardiac myocytes
present a more reduced in ammatory reaction resulting
and hyperplasia of cardiac broblasts. Critical role of the
in deletorious myocardial healing. In an experiment on
AT1 receptor subtype. Circ Res 1993;73(3):413-23.
mice it has been shown that older mice post-myocardial
3. Sadoshima J, Xu Y, Slayter HS, Izumo S. Autocrine
infarction present a more diminished in ammatory
release of angiotensin II mediates stretch-induced
response than younger the mice. is was characterized as
hypertrophy of cardiac myocytes in vivo. Cell
a reduction of neutrophils, macrophages, myo broblasts
1993;75(5):977-84.
in ltration in the damaged tissue and a reduction in the
4. Matsumoto T, Wada A, Tsutamoto T, Ohnishi M,
expression of cytokines, fouling phagocytosis and an
Isono T, Kinoshita M. Chymase Inhibition Prevents
66
Radu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
Cardiac Fibrosis and Improves Diastolic Dysfunction in
19.
Chintalgattu V, Nair DM, Katwa LC. Cardiac
the Progression of Heart Failure. Circulation
myo broblasts: A novel source of vascular endothelial
2003;107(20):2555-8.
growth factor (VEGF) and its receptors Flt-1 and KDR.
5.
Swynghedauw B. Molecular mechanisms of myocardial
J Mol Cell Cardiol 2003;35(3):277-86.
remodeling. Physiol Rev 1999;79(1):215-62.
20.
Zhou B, von GA, Ma Q, Hu YW, Pu WT. Genetic
6.
Francis GS, McDonald KM. Left ventricular
fate mapping demonstrates contribution of epicardium-
hypertrophy: an initial response to myocardial injury.
derived cells to the annulus brosis of the mammalian
Am J Cardiol 1992;69(18):3G-7G; discussion 7G-
heart. Dev Biol 2010;338(2):251-61.
9G.
21.
Kohl P. Heterogeneous cell coupling in the heart: An
7.
Volders PG, Willems IE, Cleutjens JP, Arends JW,
electrophysiological role for
broblasts. Circ Res
Havenith MG, Daemen MJ. Interstitial collagen is
2003;93(5):381-3.
increased in the noninfarcted human myocardium after
22.
Rohr S. Role of gap junctions in the propagation of the
myocardial infarction. J Mol Cell Cardiol
cardiac
action
potential.
Cardiovasc
Res
1993;25(11):1317-23.
2004;62(2):309-22.
8.
Krenning G, Zeisberg EM, Kalluri R. e Origin of
23.
Zeisberg EM, Tarnavski O, Zeisberg M, et al.
Fibroblasts and Mechanism of Cardiac Fibrosis. J Cell
Endothelial-to mesenchymal transition contributes to
Physiol 2010;225(3):631-7.
cardiac brosis. Nat Med 2007;13(8):952-61.
9.
Porter KE, Turner NA. Cardiac broblasts: At the heart
24.
Krenning G, Moonen JR, van Luyn MJA, Harmsen
of
myocardial remodeling.
Pharmacol
er
MC. Vascular smooth muscle cells for use in vascular
2009;123(2):255-78.
tissue
engineering obtained by endothelial-to-
10.
Camellitia P, Borgb TK, Kohla P. Structural and
mesenchymal transdi erentiation (EnMT) on collagen
functional characterisation of cardiac
broblasts.
matrices. Biomaterials 2008;29(27):3703-11.
Cardiovasc Res 2005;65(1):40-51.
25.
Haudek SB, Xia Y, Huebener P, et al. Bone marrow-
11.
Lijnen PJ, Petrov VV, Fagard, R H. Angiotensin II-
derived
broblast precursors mediate ischemic
induced stimulation of collagen secretion and production
cardiomyopathy in mice. Proc Natl Acad Sci USA
in cardiac broblasts is mediated via angiotensin II
2006;103(48):18284-9.
subtype 1 receptors. J Renin Angiotensin Aldosterone
26.
Isoyama S, Nitta-Komatsubara Y. Acute and chronic
Syst 2001;2(2):117-22.
adaptation to hemodynamic overload and ischemia in
12.
Katwa LC. Cardiacmyo broblasts isolated from the site
the aged heart. Heart Fail Rev 2002;7(1):63-9.
ofmyocardial infarction express endothelin de novo. Am
27.
Hasenfuss G. Animal models of human cardiovascular
J
Physiol
Heart
Circ
Physiol
disease, heart failure and hypertrophy. Cardiovasc Res
2003;285(3):H1132-H1139.
1998;39(1):60-76.
13.
Sun Y, Weber K T. Angiotensin converting enzyme and
28.
Chaturvedi RR, Herron T, Simmons R, et al. Passive
myo broblasts during tissue repair in the rat heart. J
sti ness of myocardium from congenital heart disease
Mol Cell Cardiol 1996;28(5):851-8.
and implications
for
diastole.
Circulation
14.
Desmouliere A, Redard M, Darby I, Gabbiani G.
2010;121(8):979-88.
Apoptosis mediates the decrease in cellularity during the
29.
Kai H, Mori T, Tokuda K, et al. Pressure overload-
transition between granulation tissue and scar. Am J
induced transient oxidative stress mediates perivascular
Pathol 1995;146(1):56-66.
in ammation and cardiac brosis through angiotensin
15.
Sun Y, Weber K T. Infarct scar: a dynamic tissue.
II. Hypertens Res 2006;29(9):711-8.
Cardiovasc Res 2000;46(2):250-6.
30.
Kelly D, Cockerill G, Ng LL, ompson M, Khan S,
16.
Jugdutt BI. Ventricular remodeling after infarction and
Samani NJ, Squire IB. Plasma matrix metalloproteinase-9
the extracellularcollagen matrix: when is enough enough?
and left ventricular remodelling after acute myocardial
Circulation 2003;108(11):1395-403.
infarction in man: a prospective cohort study. Eur Heart J
17.
Silzle T, Randolph GJ, Kreutz M, Kunz-Schughart
2007;28(6):711-8.
LA. e broblast:sentinel cell and local immune
31.
Spach MS, Boineau JP. Micro brosis produces electrical
modulator in tumor tissue. Int J Cancer
load variations due to loss of side-to-side cell connections: A
2004;108(2):173-80.
major mechanism of structural heart disease arrhythmias.
18.
Bosman FT, Stamenkovic I. Functional structure and
Pacing Clin Electrophysiol 1997;20 (2 Pt 2):397-413.
composition of the extracellular matrix. J Pathol
32.
Ono N, Hayashi H, Kawase A, et al. Spontaneous
2003;200(4):423-8.
atrial brillation initiated by triggered activity near the
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
67
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
pulmonary veins in aged rats subjected to glycolytic
of myocardial brillar collagen by angiotensin II. A
inhibition. Am J Physiol Heart Circ Physiol
role in hypertensive heart disease? J Mol Cell Cardiol
2007;292(1):H639-48.
2002;34(12):1585-93.
33.
Morita N, Sovari AA, Xie Y, et al. Increased
39. Lakatta EG, Levy D. Arterial and Cardiac Aging:
susceptibility of aged hearts to ventricular fibrillation
Major Shareholders in Cardiovascular Disease
during oxidative stress. Am J Physiol Heart Circ
Enterprises Part II: e Aging Heart in Health: Links to
Physiol 2009;297(5): H1594-H1605.
Heart Disease. Circulation 2003;107(2):346-54.
34.
Karagueuzian H.S. Targeting cardiac brosis: a new
40. Frangogiannis NG, Biernacka A. Aging and Cardiac
frontier in antiarrhythmic therapy? Am J Cardiovasc
Fibrosis. Aging and Disease 2011;2(2);158-73.
Dis 2011;1(2):101-9.
41. Lakatta, James B. Strait, Edward G. Aging-associated
35.
Díez J, López B, González A, Querejeta R. Clinical
cardiovascular changes and their relationship to heart
aspects of hypertensive myocardial brosis. Curr Opin
failure. Heart Fail Clin 2012;8(1):143-64.
Cardiol 2001;16(6):328-35.
42. Bujak M, Kweon HJ, Chatila K, Li N, Ta et G,
36.
Querejeta R, López B, González A, et al. Increased
Frangogiannis NG. Aging-related defects are associated
Collagen Type I Synthesis in Patients With Heart Failure
with adverse cardiac remodeling in a mouse model of
of Hypertensive Origin: Relation to Myocardial Fibrosis.
reperfused myocardial infarction. J Am Coll Cardiol
Circulation 2004;110(10):1263-8.
2008;51(14):1384-92.
37.
Cuspidi C, Ciulla M. and Zanchetti A. Hypertensive
43. Pitt B, Zannad F. e Detection of Myocardial Fibrosis
myocardial
brosis.
Nephrol Dial Transplant
An Opportunity to Reduce Cardiovascular Risk in
2006;21(1):20-23.
Patients With Diabetes Mellitus? Circ Cardiovasc
38.
González A, López B, Querejeta R, Díez J. Regulation
Imaging 2012;5(1):9-11.
68
Radu et al
CASE PRESENTATION
PRIMARY DIFFUSE LARGE B CELL LYMPHOMA OF THE HUMERUS.
CASE REPORT AND REVIEW OF LITERATURE
Oana Pobirci1, Elena Roșca2, Dumitru Decebal Pobirci3, Adela Nichita4
1Rheumatology Department, Pelican Hospital, Oradea, 2Pathological Anatomy Department, Clinical Hospital Oradea,
3Orthopedics and Traumatology Department, Hospital “Pop Mircea” Marghita, 4Radiology Department, Hospital “Pop
Mircea” Marghita, Romania
Address for correspondence:
Dr. Oana Pobirci
E-mail: oanap_30@yahoo.com
Received: 19.08.2014
Accepted: 30.09.2014
Med Con October 2014, Vol 9, No 3, 69-72
Abstract
therapeutic guidelines [3]. Due to the rarity of these
tumors there are only very few retrospective sudies
Situated among the rare bone tumors, the primary
regarding prognosis and treatment [4]. e criteria for
di use large B-cell lymphoma occupies a well-worth
the PLB include: the primary site of the tumor which
place in doctor’s attention given the di culty of
originates in the bone marrow and no other organ
diagnosis and the speci c treatment, as well as the high
involvement for six months post diagnosis [5]. PLB is a
lay time in showing of the clinical features. Biopsy
rare neoplasm and therefore the di culty in the
followed by imunohistochemistry is the gold standard
recognition and diagnosis [6].
in investigations. e presentation that follows shows a
rare case of the primary di use large B-cell lymphoma
Case Presentation
in the humerus. To the best of our knowlege this is the
rst case reported in the Romanian medical literature.
A 77 years old patient from urban area was admitted
Keywords: non-Hodgkin lymphoma, bone tumors,
to our department with pains at the right shoulder. e
immunohistochemistry
pain was profound and did not disappeared with the
administration of antialgics and secondary functional
Introduction
impairment. e physical examination revealed localised
muscle hipothony with impaired movement of the right
In Romania the bone tumors represent a 1,5% of all
shoulder and hepatomegaly 1 cm under the costal bord.
tumors followed in frequency by the genital, digestive
No peripheral lymphadenopathy was found. e rest of
and respiratory tumors. Primary lymphoma of the bone
his physical examination was within the normal limits.
(PLB) originates in the medulary cavity and presents as
Originally he was diagnosed as having an in ammatory
a single and localised lesion. It represents aproximately 3
process with blood erythro-sedimentation 16mm/hour
% of the malignant bone tumors and 1% of the
but with negative C reactive protein. Chest X-Ray was
malignant lymphomas [1]. PLB was for the rst time
normal. e radiografy of the right shoulder showed
described by Oberling in 1928 [2] and is an extremely
osteolysis at the proximal right humerus 5X4 cm in size
rare disease so there are no established speci c
(Figure 1).
Primary Diffuse Large B-Cell Lymphoma of the Humerus. Case Report and Review of Literature
69
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
A
B
Figure 1. e radiological
Figure 2. Primary di use large B-cell lymphoma of the humerus.
examination of the right scapular-
A. Di use proliferation of large lymphoid cells within
humeral articulation presents a
a hypocellular stroma (H&E x100).
zone of osteolysis at the right
B. Di use large lymphoid cells with large nuclei (HE, 400X)
proximal humerus and with
prominent cortical distruction
For the establishment of the diagnosis an explorative
biopsy of the tumor was performed. e histological
examination of the tumor fragment revealed a di use
in ltration of relatively large cell size.
e tumor cells
had round nuclei which appeared vescicular with no
prominent nucleoli.
e cytoplasm was moderately
abundant (Figure 2, A and B). Immunohistochemical
stains for common leucocytic antigen (LCA) and CD
20 resulted positive in the tumor cells (Figure 3).
In order to exclude a metastatic carcinoma
cytokeratin AE 1 and AE 3, CK 7, CK 20, TTF-1 were
perfomed and resulted negative in the tumor cells.
Figure 3. Primary di use large B-cell
Neuroencocrine markers, chromogranin, sinaptophysin
lymphoma of the humerus. Strong CD 20
and neuro speci c enolase (NSE) were negative as well.
positivity of the tumor cells (x40)
e LCA and CD 20 positivity along with the celular
morfology, con rm the diagnosis of primary di use
large B-cell lymphoma of the humerus. e patient was
Table I. Primary lymphomas of the humerus, years 1970-2014
transfered to the oncology department for speci c
Author
Year
Country Nr of cases
treatment.
De Santis E et al.[10]
1987
Italy
1 case
Pettit CK et al. [6]
1990
USA
2 cases
Blasius S et al. [11]
1992
Germany
6 cases
Discussions
Arredondo J et al. [12]
1999
USA
1 case
Neben K et al. [13]
2001
Germany
1 case
e clinical presentation of this case was initially a
Moazzam N et al. [14]
2002
USA
1 case
tumor of the humerus.
e imaging investigation
Stemberga V et al.[15]
2003
Croatia
1 case
revealed no other pathologies and no lymphadenopathy.
Robinson Det al. [16]
2003
Israel
1 case
Due to the site of the tumor it was thought to be an
Bralić M et al. [17]
2008
Croatia
1 case
Wong T et al. [18]
2008
Taiwan
1 case
osteosarcoma.
e morpholgy along with the
Marotta D et al. [19]
2008
Italy
1 case
immunohistochemical negativity CK20, CK7 and
Mondal SK et al. [20]
2011
India
1 case
TTF-1
(thyroid transcription factor
1) excluded
Li ZS et al. [21]
2011
China
1 case
osteosarcoma and metastatic carcinoma.
Caporale MF et al. [9]
2013
Italy
1 case
e morphological features of the tumor cells raised
Mondello P et al. [3]
2014
Italy
1 case
the possibility of a neuroendocrine tumor but with the
Ben Salah H et al. [22]
2014
Tunis
4 cases
NSE, chromogranin and sinaptophysin negativity it was
Pobirci O et al.
2014
Romania
1 case
70
Pobirci et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
exluded as well. e di use pattern with LCA and CD-
8.
Mika J, Schleicher I, Gerlach U, Adler CP, Uhl M,
20 positivity established the diagnosis of primary di use
Knoeller SM. Primary bone lymphomas thought to be
large B-cell lymphoma.
osteomyelitis urgently demand a rapid diagnosis in bone
Primary bone lymphoma is a rare entity. e patient
pathology. Anticancer Res 2012;32(11):4905-12.
sometimes complain about local pain, with swelling of
9.
Caporale MF, Gambino GF, Larosa FS, Del Buono A,
the region.
e patological fractures of the femur and
Di Segni F. Non-Hodgkin’s lymphoma: unexpected cause
humerus are well documented in literature; however
of shoulder pain. A systematic review of the literature.
primary lymphoma at these sites are rare [7]. e delay
Muscles Ligaments Tendons J 2013;3(3):236-9.
in clinical symptoms represents a di culty in the
10.
De Santis E, Di Giovanni C, Pallotta F. Primary
diagnosis.
e delay in diagnosing these cases can have
reticulosarcoma of bone (non-Hodgkin’s lymphoma). A
serious impact on the outcome [8].
study of
12 cases. Ital. J OrthopTraumatol
Revising the di use B-celllymphomas published in
1987;13(4):477-84.
literature since
1970 until present, we discovered 25
11.
Blasius S, Edel G, Vestring T, Ueda Y, Wuisman P,
cases, ours being the 26th (Table I).
Böcker W, Roessner A. Non-Hodgkin’s lymphoma with
primary osseous manifestation, from the les of the Bone
Conclusions
Tumor Registry of Westphalia. Verh Dtsch Ges Pathol
1992;76:146-50.
e diagnosis of the bone tumors always requires an
12.
Arredondo J, Worland R, Sinnenberg R, Qureshi G.
interdisciplinary cooperation of the clinitions,
Non- Hodgkin’s lymphoma as an unexpected diagnosis in
radiologist and anatomo-pathologist.
a shoul- der arthroplasty. J Arthroplasty 1999;14:108-
To the best of our knowledge this is the rst case in
11.
Romania.
13.
Neben K, Werner M, Bernd L, Ewerbeck V, Delling
G, Ho AD. A man with hereditary exostoses and high-
grade non-Hodgkin’s lymphoma of the bone. Ann
References
Hematol 2001;80(11):682-4.
14.
Moazzam N, Malik AA, Potti A. B-cell lymphoma
1.
Singh T, Satheesh CT, Lakshmaiah KC, et al. Primary
mimicking multiple myeloma. Leuk Lymphoma
bone lymphoma: a report of two cases and review of the
2002;43(9):1869-73.
literature. J Cancer Res er 2010;6:296-8.
15.
Stemberga V, Dobi-Babić R, Bosnar A, et al. Primary
2.
Heyning FH, Hogendoorn PC, Kramer MH, et al.
non-Hodgkin lymphoma of the humerus following
Primary non-Hodgkin’s lymphoma of bone: a
traumatic injury: case report. Hematol Oncol 2003;
clinicopathological investigation of 60 cases. Leukemia
21(3):109-14.
1999;13:2094-8.
16.
Robinson D, Halperin N, Agar G, Alk D, Rami K.
3.
Mondello P, Mian M, Arrigo C, Pitini V. Primary
Shoulder girdle neoplasms mimicking frozen shoulder
di use large B-cell lymphoma of the bone: bendamustine
syndrome. J Shoulder Elbow Surg 2003;12:451-455.
and rituximab are able to overcome resistant disease.
17.
Bralić M, Stemberga V, Cuculić D, et al. Primary non-
Springerplus 2014;3:342.
Hodgkin’s lymphoma of the humerus presenting as
4.
Lakshmaiah K, Guruprasad B, Purohit S, Rao S,
osteomyelitis. Coll Antropol 2008;32 Suppl 2:229-31.
Bishwas S, Lokanath D. Primarynon-Hodgkin’s
18. Wong T, Ko JY, Wang FS, Chen YJ, Ma MC. Epstein-
lymphoma of bone: poly-ostotic versus mono-ostotic
Barr virus associated extranodal natural killer T cell
ubtypes. Ecancermedicalscience 2013;7:330.
lymphoma of nasal type mimicking pyogenic osteomyelitis
5.
Mulligan ME, McRae GA, Murphey MD. Imaging
of the proximal humerus. Chang Gung Med J
features of primary lymphoma of bone. AJR Am J
2008;31(3):314-9.
Roentgenol 1999;173:1691-7.
19. Marotta D, Sgambato A, Cerciello S, et al. Soft tissue
6.
Pettit CK, Zukerberg LR, Gray MH, et al. Primary
non-Hodgkin lym phoma of shoulder in a HIV patient:
lymphoma of bone. A B-cell neoplasm with a high
a report of a case and review of the literature. World J
frequency ofmultilobated cells. Am J Surg Pathol
Surg Oncol 2008;6:111.
1990;14(4):329-34.
20. Mondal SK, Bera H, Biswas PK, Mallick MG. High-
7.
Siddiqui YS, Khan AQ, Sherwani M. Pathological
grade plasmablastic neoplasm of humerus in an HIV-
Fractures in Primary Non-Hodgkin’s Lymphoma of the
negative patient, which was indeterminate between
Bone: A Case Series with Review of the Literature. J
plasmablastic lymphoma and plasmablastic myeloma. J
Clin Diagn Res 2013;7(3):513-7.
Cancer Res er 2011;7(2):214-6.
Primary Diffuse Large B-Cell Lymphoma of the Humerus. Case Report and Review of Literature
71
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
21. Li ZS, Li PF, Wang Z, Huang GS. Primary extranodal
22. Ben Salah H, Fourati N, Elloumi M, Boudawara T,
soft-tissue B-cell lymphoma with abundant immunoglobulin
Frikha M, Daoud J. Localized primary bone
inclusions mimicking adult rhabdomyoma: a case report. J
lymphoma: about four cases. Cancer Radiother
Med Case Rep 2011;7(5):53.
2014;18(1):23-7.
72
Pobirci et al
CASE PRESENTATION
REPLANTATION OF AMPUTATED FINGERS AFTER RING AVULSION.
TECHNICAL CONSIDERATIONS AND FUNCTIONAL PROGNOSIS
RESULTS
Doina Prisecari1, Dragoș Zam rescu2, Șerban-Arghir Popescu2, Ioan Lascar2, Alisa Zisman1, Alexei Prisecari3
1Clinic of Plastic Surgery and Reconstructive Microsurgery, Emergency Clinical County Hospital “Sf. Apostol Andrei”,
Constan a, România, 2Clinic of Plastic Surgery and Reconstructive Microsurgery, București Emergency Clinical Hospital,
University of Medicine and Pharmacy ”Carol Davila”, București, Romania, 3Clinic of Orthopaedic-Traumatology,
Emergency Clinical County Hospital “Sf. Apostol Andrei”, Constan a, România
Address for correspondence:
Prisecari Doina
Spitalul Clinic Jude ean de Urgen ă “Sf. Apostol Andrei”
B-dul Tomis nr 145, CP 900591, Constan a
Tel 0742707124
Email: doinaschipor@yahoo.com
Received: 02.09.2014
Accepted: 30.09.2014
Med Con October 2014 Vol 9, No 3, 73-77
Abstract
Results:
9 patients were grouped in this study.
Survival rate was 57% for complete amputated ngers
Avulsion amputations constitute a severe problem
and 43% for partial amputations.
because of signi cant lesions in nerves and vessels. Both
Keywords: nger avulsion, nger amputation,
arterial and venous anastomoses are relevant factors,
hand surgery outcomes, replantation, revascularization
which determine the success in replantation of avulsed
ngers. Surgical experience in vessel dissection, election
Introduction
of venous and nervous grafting as reconstruction
methods are as well of considerable importance.
e appearance of microsurgical techniques
Purpose: e goal of this research was to assess the
constituted a big step forward for amputated and
survival and functional rates in nger replantations after
avulsed nger replantations.
e type of lesions
complete or partial amputations through avulsion
produced in avulsions represent a signi cant problem,
mechanism.
also hard to manage as treatment, because of a complex
Methods: e followed criteria were used in this
skin, vascular and nervous involvement.
study: 1. Complete/partial nger amputations at the
Replantation/reperfusion of amputated
nger
level of proximal phalange or distal to the proximal
through an avulsion mechanism is the most delicate
interphalangial joint.
2. Elected surgical treatment:
contest in hand surgery and failure is not a rare condition.
replantation or microsurgical reperfusion
- arterial
After a series of replantations in such cases, we could
followed by venous anastomosis (in a direct manner or
draw the conclusion that the replantation of a degloved
with venous grafting).
3. Two point discrimination
segment was successful when the blood vessels included
sensation obtained after replantation/revascularization -
in avulsed skin didn’t have lesions at multiple levels or
equivalent to a functional result.
they were complete destroyed (we are talking also about
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
73
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
the peripheral circulation which in such type of traumatic
stump. e quality of blood vessels is evaluated under OM
mechanism may be irreversible closed). Although
and the edges are cut in healthy tissue. After bone xation
replantated ngers recover some function, such an aim
and tendon repair, arterial anastomosis is performed using
was proved to be hard to realize. at’s why indications
9.0-10.0 prolene suture. Venous anastomosis is done in a
and contraindications for surgery candidates in degloving
termino-terminal manner or interposing venous grafts
amputated ngers continued to evolve to exclude those
where the tension occur using 10.0-11.0 prolene suture.
with a bad functional prognosis from the very beginning.
After successful reperfusion loose skin suture is executed.
e surgeons continued to extend the limits of
microsurgery. ere were implemented new techniques
Results
to manage the di culties in order to save avulsed ngers.
Avulsed lesions are usually quoted as the type of
Our report includes a total of 9 cases of amputations
injuries with unsatisfactory functional results [1,2,3],
through avulsion, 4 of which were complete and 5 partial.
mainly in complete amputations or with associated joint
ere were registered 2 cases of total failure (1 female and
destruction. Recent studies showed good functional
1 male), 3 cases of partial failure (partial necrosis which
results after avulsed nger replantations, even though,
were solved by future surgeries).
1 patient needed a
contesting these recommendations [6].
venous graft in order to perform the anastomosis, in 2
e purpose of this study is to make a systematic
patients an arthrodesis was needed at the level of proximal
analysis of avulsed nger replantations in order to o er
interphalangeal joint and 1 at the distal interphalangeal
reliable evidence in rates of survival and functionality.
joint. In all cases only one vein was repaired and in 3 cases
Secondary objective was to compare functional results
venous grafting was needed. Out of all successful cases
after avulsed nger replantations to the results obtained
just one showed signs of poor venous ow and medicinal
in replantation of amputated ngers in the second zone
leeches were used ( Figure 3 A,B,C,D,E,F). None of the
with exor tendon and digital nerve repair. e overview
patients did need blood transfusion.
of functional results obtained with these two methods,
All patients were followed up at 3, 6 and 12 months.
forms the ground for future comparison.
Every one of them was satis ed with the functional
results achieved. None did ask for late amputation
Methods and Materials
because of the esthetics of the nger, neuromas, rigidity,
cold intolerance.
e purpose of this study was to show that this
Medium range of motion at interphalangeal joints
method of microsurgical replantation/reperfusion
was 135º for complete amputations and 160º in partial
actually can be successful in avulsed nger replantations.
amputations. Protective sensibility was recovered in all
During
2007-2010
9 replantations of complete or
the cases. Every patient of the group study was socially
partial amputations through avulsion were performed.
and professionally rehabilitated after an average period
ere were 6 female, 3 male; 26-59 years of age; under
of 3-4 months.
ring block anesthesia.
All of patients were right handed.
e a ected
Discussions
ngers were: left ring nger in 4 patients, policis in 2
patients
(Figure 1 A,B,C,D) and index/medius in 3
Replantation/reperfusion after amputation through
patients (Figure 2 A,B,C,D).
an avulsion mechanism are usually for the poor
Complete amputations at the level of proximal
functional results [1,2,3,7], particularly after complete
interphalangeal joint were noticed in 2 cases and 1 case at
amputation or when associated bone, joint, soft tissue,
the level of distal interphalangeal joint.
e successfully
vascular, nervous destruction was present [5,7].
replantated ngers were drained by one venous anastomosis
In cases when venous grafting was used to restore
(direct/venous graft). In all cases local anesthesia was used
venous blood out ow, controlling the permeability of
associated with a Tourniquet at the base of the nger.
the anastomosis and sometimes revising it was usually
When starting the procedure the amputated part is
done. Only after that, repair of other injured structured
examined under operative microscope (OM) rst. An
was performed.
is simple, easy and rapid method
unique longitudinal incision is done on the volar side for
permitted the overview of twisted, convoluted grafts.
identi cation of nerves and arteries. It is important to avoid
Tendon, nervous, venous grafting allows for good
making two incisions, because of high risk of necrosis of
functional results even in such cases of amputation through
the skin in between those two. Arteries and veins are
avulsion. Subcutaneous vein harvesting represented a
marked on the amputated part and also on the remnant
simple and quick repair technique in such cases [4].
74
Prisecari et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
A
B
C
D
Figure 1. A,B. Complete amputation through avulsion of policis with long exor,
extensor tendon avulsion. C,D. 1 year follow-up view
A
B
C
D
Figure 2. A,B. Index avulsion properative view. C,D. Postop view
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
75
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
A
B
C
D
E
F
Figure 3. A. Female with avulsion trauma and complete amputation at the level of distal
interphalangeal joint of small digit with profound exor avulsion. B. Arthrodesis at the
proximal interphalangeal joint of the small nger with Kirschner axial pin. C,D. Postop view.
E. 72 hours view, poor venous out ow with the use of medicinal leeches. F. 3 months view
Conclusions
e use on a large scale of venous grafting techniques
for venous out ow in traumas through avulsion with
Generally, the prognosis after amputation through
complete amputations, increases the rates of success and
avulsions is rather reserved compared to those through
may keep the length of the nger.
cutting mechanism. e recovery of function is reduced
Given the type of injury, most of patients necessitate
and the number of complications is higher than in the
secondary surgical procedures.
avulsion amputations. Nervous regeneration is close to
zero because of the elongation/avulsion mechanism of
injury. In time patients develop a type of sensibility
References
called protective sensibility. Functionally speaking,
range of active/passive motion is recovered near 50%.
1. Boulas HJ. Amputations of the ngers and hand:
Even with bad functional recovery, keeping the
indications for replantation. J Am Acad Orthop Sur
nger meant an important factor in maintaining an
1998;6:100-5.
optimal level in quality of life, especially for children
2. Pederson WC. Replantation. Plast Reconstr Surg
and female patients.
2001;107:823-41.
76
Prisecari et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
3. Urbaniak JR, Roth JH, Nunley JA, Goldner RD,
6. Akyurek M, Safak T, Kecik A. Ring avulsion
Koman LA. e results of replantation after amputation
replantation by extended debridment of the avulsed
of a single nger. J Bone Joint Surg Am 1985;67:611-9.
digital artery and interposition with long venous grafts.
4. Adani R, Marcoccio I, Castagnetti C, Tarallo L. Long-
Ann Plast Surg 2002;48(6):574e81.
term results of replantation for complete ring avulsion
7. Ross DC, Manktelow RT, Wells MT, Boyd JB.
amputations. Ann Plast Surg 2003;51:564-8.
Tendon function after replantation: prognostic factors
5. Urbaniak JR, Evans JP, Bright DS. Microvascular
and strategies to enhance total active motion. Ann Plast
management of ring avulsion injuries. J Hand Surg Am
Surg 2003;51:141-6.
1981;6:25-30.
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
77
Photos from Medical Days of Satu Mare, 11th Edition
HISTORY OF MEDICINE
CONSTANTIN STANCA 1889 1969 A PRESTIGIOUS
GYNECOLOGIST AND ONCOLOGIST OF THE 20TH CENTURY
Cristian D. Barsu
Department of History of Medicine, Social Sciences and Humanities, “Iuliu Ha ieganu” University of Medicine and
Pharmacy, Cluj-Napoca
Address for correspondence:
Dr. Cristian D. Barsu
31 Avram Iancu Street, 400083, Cluj-Napoca, România
Email: cristianbarsu@yahoo.com
Received: 14.08.2014
Accepted: 15.09.2014
Med Con October 2014, Vol 9, No 3, 79-82
Abstract
development of Romanian medicine, especially in the
rst half of the 20th century. He was the rst Director of
Dr. Constantin Stanca (1889-1969) was a prestigious
the Institute for the Study and Prevention of Cancer
personality of the 20th century in Romanian gynecology
(later being renamed as the Institute of Oncology) from
and oncology. He was the rst director of the Institute for
Cluj, between 1929 and 1940. e initiative for creating
the Study and Prevention of Cancer in Cluj between 1929
it was elaborated by Prof. Dr. Iuliu Moldovan (1882-
and 1940. ere he founded and directed the Gynecologic
1966), who was also its honorary director in 1929. is
Oncology Surgery Department. Also he created the
Institute was the rst in Romania and among the rst
Department of Radiotherapy and a Laboratory of
three of Europe. It’s useful to mention that until 1947
Experimental Cancer at the same Institute. Another of his
the surname of the Institute was “Iuliu Maniu”, because
achievements was the foundation of the rst cancer review
in 1929 Iuliu Maniu, as the Romanian prime minister,
in Romania, named “ e Cancer”, which existed from
assisted in its foundation. C. Stanca founded the
1932 until 1938. In addition, he realized the rst Romanian
Gynecologic Oncologic Surgery Department, the
lm on the subject of cancer, which was lmed in his
Department of Radiotherapy and the Laboratory of
Institute. C. Stanca founded an important school of
Experimental Cancer, the latter which were exceptionally
oncology and gynecology in Transylvania, characterized by
modern for the interwar level of medicine.
professionalism, style, surgical radicalism and demonstrating
is paper is published in 2014, to mark 85 years
especially good results for the interwar period.
since the Oncological Institute was created in Cluj.
Keywords: Constantin Stanca, gynecology, oncology,
Institute for the Study and Prevention of Cancer from
Stanca’s life and career
Cluj.
Constantin Stanca was born on
16 September
Introduction
1889, at Petroşani. He and his older brother Dominic
Stanca (1892-1979), as well as one of his nephews
e gynecologist and oncology surgeon Constantin
Octavian Stanca (1908-1977) became physicians. It is
Stanca
(1889-1969) had an important role in the
necessary to point out that during the 20th century -
Constantin Stanca (1889-1969) - A Prestigious Gynecologist and Oncologist of the 20th Century
79
HISTORY OF MEDICINE
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
and even at present - that in some presentations a
of discipline of the Faculty, […] and spreading false data”
confusion persists between Constantin and Dominic
[4]. If indeed it was only a pretext, then C. Stanca must
Stanca.
have been appreciated to be from an early stage of his
In creating Stanca’s family history, the well known
career, a very valuable gynecologist and had the courage
medico-historian Prof. Dr. Valeriu Bologa (1892-1971)
to expose and support his views.
evidenced that: “A family of scholars from the Hunedoara
His career continued in 1920 as a primary physician
district, whose genealogical lineage started with Stanca, the
at the Women’s Hospital in Cluj.
is hospital was
father, and was continued by sons and grandchildren [who
organized and led by his brother Dominic Stanca, who
became] scientists, writers and pillars of communities; a
was also a worthy gynecologist. e Woman’s hospital in
family who was always present, for a period of eighty years,
Cluj was the rst gynecological hospital organized by the
realizing much for Transylvania in preparation for the
Ruling Council of Transylvania, immediately after the
Great Union” [1]. For marking in a more important way
Great Union of Transylvania to the Romanian Kingdom.
the prestige of Stanca’s family, V. Bologa added that “in
Being eager for his professional development, in 1924
history, medicine and literature, Stanca’s name is seen and
Constantin Stanca became PhD at the Bucharest Faculty
heard over three generations” [1].
of Medicine, with the thesis
“Fundamental lines in
Constantin Stanca was a student at the Hungarian
gynecological and obstetrical semiology and propedeutics”.
Faculty of Medicine in Cluj. One of his most important
For eight years, from 1921 to 1929, he was the director of
professors was D. Szabó, who was the director of the
the Red Cross State Sanatorium in Cluj.
Gynecologic Clinic between 1892 and 1918. Stanca
During the same period, he had the occasion to
graduated from the Faculty in 1914 and become a
improve his professional training in Vienna, at the
Doctor in Medicine and Surgery a few months after
Gynecological Clinic led by the famous Prof. Dr. Ernst
graduation. In the same year he began his didactic career
Wertheim (1864-1920) and then by Prof. Dr. Fritz
in the same Faculty, at the Anatomy Department.
Kermauner (1872-1931). Also Stanca expanded his
Liking clinical medicine, he was transferred as assistant
surgical techniques at the Surgery Clinic in Vienna,
to the Cluj Clinic of Gynecology. Here he was present
directed by Prof. Dr. Anton von Eiselberg (1860-1939).
until 1919, when the Hungarian Faculty of Medicine in
e most important part of C. Stanca’s career took
Cluj stopped its activity.
place at the Institute for the Study and Prevention of
It is interesting to mention the fact that in 1919 May
Cancer “Iuliu Maniu” from Cluj. Under the guidance of
12, Alexandru Nemeş together with C. Stanca and
Prof. Dr. Iuliu Moldovan, the founder of this Institute,
Coriolan Tătaru
(1889-1957) were nominated to be
Stanca became its director in
1929 and essentially
members of the group which had to take over the
contributed to its organization. He set up the
University Clinics from Cluj, “Carolina Hospital” and
gynecologic oncology surgery department, the
other pending institutes belonging to the old Faculty of
department of radiotherapy and a laboratory of
Medicine for the Romanian State. is mission was given
experimental cancer.
to them by Onisifor Ghibu (1883-1972) - the delegate of
Another achievement was the foundation of the
the Ruling Council of Transylvania for this task [2].
rst oncologic review in Romania. is review, named
During the academic year 1919/1920 C. Stanca was
“Cancer”, existed from 1932 until 1938. At that time it
assistant at the Clinic of Gynecology, which belonged to
was very di cult to create a special periodical focused
the Romanian Faculty of Medicine in Cluj.
on oncology. e rst reason was that the theoretical
As a result of the con ict between some university
level in this eld was not yet very developed. e second
assistants and the director of the Gynecological Clinic
was that there were not many physicians from the
- Prof. Dr. Cristea Grigoriu (1883-1951), on the 1
Institute for the Study and Prevention of Cancer from
April 1920, the Professorial Council of Cluj Medicine
Cluj who had time to write scienti c articles about their
Faculty - directed by the Dean Iuliu Ha ieganu (1885-
experience in oncology. But nally the insu ciency of
1959), decided to dismiss Dr. Alexandru Nemeş and
nancial support for its publication contributed to its
Dr. Constantin Stanca, together with other three
demise. Considering these conditions, the fact that
residents [3]. After more than nine decades it is di cult
“Cancer” review existed seven years can be considered a
to ascertain whether the reason given by Prof. Grigoriu
performance for Romanian medicine during the rst
for his decision was a real one or was, as a matter of fact,
half of the 20th century and an important achievement
only an excuse to eliminate a part of the valuable young
for European medicine during the same period.
physicians from the sta of the Gynecological Clinic.
Stanca created the rst Romanian lm with an
Grigoriu’s accusation was: “the infringement of the rules
oncology topic. is lm, realized in the Institute where
80
Barsu
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
HISTORY OF MEDICINE
he was Director had an important educational role,
fallopian tube cancer” („Cancerul tubar primiv”) (1922),
both for the public, as well as for physicians [5].
“New researches concerning the painful re ex at distance”
He was interested both in nursing sick cancer
(„Noi cercetări în re exul dureros la distan ă”) (1927),
patients, scienti c research, teaching and also in
“Ovarian grafts”
(„Grefele ovariene”)
(1931),
“About
founding oncologic units in the region [6].
totally enlarged hysterectomy for uterine cancer made
It is useful to mention that in the same time when
between 1924 and 1935” (“Asupra histerectomiilor totale
he was Director of the Institute for the Study and
lărgite pentru cancerul uterin, pe anii 1924-1935”) (1935),
Prevention of Cancer, C. Stanca continued to work at
“ e pathological connection between cancer of the
the “Women’s Hospital” in the same town.
appendix and ovaries” („La connexion pathologique entre
Wanting to have a more important formative role for
le cancer de l’apendice et les ovaries”) (1935), “Spontaneous
students and young physicians, in
1938 he became
cervical amputation during pregnancy”
(„Amputa ia
Assistant Professor at the Gynecological Clinic of the
spontană a colului uterin în cursul sarcinei”) (1939) etc.
Faculty of Medicine from Cluj. It is strange that the same
He published the results of his research in reviews in Cluj,
director - Prof. Grigoriu - who had dismissed C. Stanca
Bucharest, Vienna, Leipzig, Paris, Buenos Aires etc.
from the sta of the Clinic 18 years before, changed his
He was founder member of the Society for Gynecology,
opinion and allowed Stanca to have an important job in
Obstetrics and Endocrinology, created in 1935 at Cluj and
the same Clinic. Was it the result of Grigoriu’s remorse? It
directed by Cristea Grigoriu. C. Stanca was corresponding
is very di cult to know the real cause.
member of the French Society for Gynecology and
In his entire career which took place at Cluj between
honorary member of the Association Against Cancer from
1929 and 1940, Stanca founded “a strong gynecologic
Buenos Aires. He was also vice-president of the Physicians’
oncology school, which was distinguished by radicalism,
General Association from Romania [11].
professionalism, surgical style and by especially good results
During his career, he was awarded with many
for that period”, as Ilie Neam u (1910-?) pointed out [5].
medals, such as: „Ferdinand Order” - in the degree of
It is useful to mention that I. Neam u was one of the
Knight, „Romanian Crown” - in the degree of Knight
best pupils from C. Stanca and in the ’70’s directed the
and of Commander, ”Queen Mary” Cross (1942) and
Section of the Surgery and Gynecology of the Oncologic
„Sanitary Merit” - First Class.
Institute from Cluj.
C. Stanca remained in the memory of those who
At the outbreak of the Second World War, in
knew him as a remarkable physician, who had a long
September 1940 C. Stanca left Cluj and established
career, with many achievements.
himself in Bucharest. ere he continued to work hard.
His nephew - the writer Horia Stanca (1909-2002)
In 1941, he remained o cially Associate Professor at
wrote in his memories entitled “Fragmentarium from
the Cluj Faculty of Medicine, which was in refuge in
Cluj” that: C. Stanca had ”agile hands with thin [...]
Sibiu. But his principal activity took place at the “Prince
ngers, [with which he] worked with a pungency that lled
Nicolae” Hospital in Bucharest, where he was appointed
me with wonder for his skill in handling instruments and
primary physician. He tried to transform this hospital
in locating them in the right places in the [patient’s] body”
into an oncologic institute, but it was impossible during
[12].
the war, when it was an immense need for hospitals for
soldiers. Meantime, he was consultant physician for
prenatal diseases at the Social Insurance Department
References
[7]. In 1948 he set up the Maternity Unit of the “Ilie
Pintilie” - Pantelimon Hospital. ere he was director,
1. Bologa VL. Un înfăptuitor: Constantin Stanca (1889-
gynecologist and obstetrical surgeon [8].
1969). În Restituiri, Ed. Med. Univ.
“Iuliu
C. Stanca succeeded to impose himself professionally
Ha ieganu”, Cluj-Napoca, 2009:44-45.
and he was awarded with the title “Honorary Professor”.
2. Ghibu O. La a douăzecea aniversare a Universită ii
en, in
1960 he was awarded with the “Physician
Dacia Superioară, edi ia a II-a, îngrijită, revăzută, cu
Emeritus” distinction [9].
us, in 1961/1962 he was
prefa ă de Prof. Dr. Doc. Crişan Mircioiu, Ed.
Professor of obstetrics and gynecology at the Bucharest
Napoca Star, Cluj-Napoca, 2001:54.
Faculty of Medicine [10].
3. Bârsu C. Reuniunea Consiliului profesoral al Facultă ii
e scienti c activity of Constantin Stanca included
Româneşti de Medicină din Cluj din 1 Aprilie 1920. În
more than
100 scienti c works, published or
Mărturii ale începutului Facultă ii de Medicină din
communicated, the majority having an oncologic pro le.
Cluj, 1919-1920, Ed. Med. Univ. „Iuliu Ha ieganu”,
Among these are included the following papers: “Primary
Cluj-Napoca, 2004:139.
Constantin Stanca (1889-1969) - A Prestigious Gynecologist and Oncologist of the 20th Century
81
HISTORY OF MEDICINE
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
4. Bârsu C. Întrunirea Consiliului Profesoral al Facultă ii
8. Ministerul Sănătă ii. Direc ia Eviden ei Documentării
Româneşti de Medicină din Cluj din 23 Aprilie 1920.
Statistice. Anuarul medicilor 1948, Monitorul O cial
În Mărturii ale începutului Facultă ii de Medicină din
şi Imprimeriile Statului. Imprimeria Centrală,
Cluj, 1919-1920: 141.
Bucureşti, 1948:499.
5. Neam u I. Profesor Dr. Constantin Stanca (1889-1969).
9.
*** Constantin Stanca. În Enciclopedia medicală
În Enciclopedia Oncologică: Cancerul. colului uterin.
românească, de la origini până în prezent, sub red.
Material de documentare şi îndrumare metodologică, sub
Ursea N., vol. 4, Ed. Univ. “Carol Davila”, Bucureşti,
red. Chiricu ă I. Într. Poligr. Cluj-Napoca, 1976:227,
2009:2780-2781.
228
10.
*** Lista profesorilor şi conferen iarilor în anul universitar
6. Chiricu ă I, Bolba Gh. Activitatea complexă a
1961/1962 la Facultă ile de Medicină, Stomatologie şi
Institutului Oncologic Cluj-Napoca, în
guri şi
Specializare şi Perfec ionare. În Învă ământul Medical şi
comentarii:
1929-1979. În Enciclopedia Oncologică,
Farmaceutic din Bucureşti. De la începuturi până în
vol.
7, Cancerul sânului. Experien a românească.
prezent, sub red. Ilea T, Ghelerter I, Du escu B, Bercuş
Semicentenarul Institutului Oncologic Cluj-Napoca.
CI, Într. Poligr. „Arta Gra că”, Bucureşti, 1963:566.
Material de documentare şi îndrumare metodologică,
11.
*** Facultatea de Medicină. În Anuarul Universită ii
Într. Poligr. Cluj-Napoca Cluj-Napoca, 1981:662.
„Regele Ferdinand”, Ed.
„Cartea Românească din
7.
*** Anuarul general al medicilor din România. 1941.
Cluj”, Sibiu, 1943:663-664.
Cu datele recensământului din 15 martie 1941, Tipogr.
12. Stanca H. Anii de universitate. În Fragmentarium
„Universul”, Bucureşti, 1941:256.
Clujean, Ed. „Dacia”, Cluj-Napoca, 1987:87.
82
Barsu
GUIDANCE FOR DRAWING UP
GUIDANCE FOR AUTHORS
Scope
on which patients or other subjects of your experiments
e Medical Connections publishes papers reporting
clearly grant permission for the publication of
original clinical and scienti c research, which contribute
photographs or other material that might identify them.
to the advancement of knowledge in all eld of medicine.
If the consent form for your research does not speci cally
e journal also publishes reviews, editorials and short
include this, please obtain it or remove the identifying
communications on speci c topics. Case reports will be
material. A statement must be included in the ‘Methods’
accepted if of great interest and well investigated. Letters
section of your paper.
to the Editor, especially those mentioning an opinion on
an article previously published, or expressing a new
Ethics Committee approval
nding are welcome. e website address of the Medical
You must state clearly in your submission in the
e
Methods section that you conducted studies on human
journal is published quarterly and papers are accepted
participants with the approval of the Hospital, or
for publication in English language. Papers from
University Ethics Committee etc. Similarly, you must
contributors living abroad and from Romanian authors
con rm that experiments involving animals adhered to
should be addressed to the editorial o ce: dr. Bumbulu
ethical standards.
Călin, assitant editor in chief of Medical Connections,
Eroilor Revolu iei Pl. no.23-440055 Satu Mare,
Copyright assignment
Romania. Tel./Fax:
+40-261-710456,
e-mail:
Papers are accepted for publication on the
bumbulutcalin@yahoo.com.
understanding that exclusive copyright in the paper is
assigned to the Publisher. Authors may use material
Redundant or duplicate publication
from their paper in other works published by themselves.
We ask you to con rm that your paper has not been
published in its current form or a substantially similar
Submissions
form, that it has not been accepted for publication by
All manuscripts submitted to the Medical
another journal, and that it is not under consideration
Connections are made available for online review.
e
by another publication.
journal introduced the electronic submission of
manuscripts in Word format, but also accepts
Conflicts of interest
manuscripts submitted as attachments to electronic
We ask authors to state all possible con icts of
mail (text, gures and tables). Do not send them in
interest, including nancial and other relationships. If
PDF format. e word count for electronic submissions
you are sure that there is no con ict of interest, please
is up to 3,500 words for original articles, 2,500 words
state this also.
e sources of funding should be
for case reports, 2,000 for clinical imaging papers, 500
acknowledged in your paper.
words for letters, and 4,500 words for review articles.
Authors should NOT in addition post a hard copy
Permissions to reproduce previously
submission to the editorial o ce, unless they are
published material
supplying artwork, letters or if les that cannot be
Please send us copies of permission to reproduce
submitted electronically, or have been instructed to do
material (such as illustrations) from the copyright holder.
so by the editorial o ce. For those authors who have no
option but to submit by mail please send one copy of
Patient consent forms
the article, plus an electronic version on CD-ROM to
e protection of a patient’s right to privacy is
the Editorial O ce, Conexiuni Medicale/Medical
essential. Please send copies of patient’s consent forms
Connections, Eroilor Revolu iei Pl. no.23-440055 Satu
83
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Mare, Romania. Double spacing should be used
Review articles and case reports should include an
throughout the manuscript, which should include the
unstructured summary.
following sections, each starting on a separate page: title
Key words
page, abstract and key words, text, acknowledgements,
e abstract should be followed by a list of 3-10
references, individual tables and legend for gures. Pages
keywords or short phrases which will assist the cross-
should be numbered consecutively, beginning with the
indexing of the article and which may be published.
title page, and the Arabic numbers should be placed in
When possible, the terms used should be from the
the top right hand corner of each page.
Medical Subject Headings 262 list of Index Medicus
Presentation of papers
Text
Title page
Full papers of an original study may be divided into
e title page should carry the full title of the paper
sections headed Introduction, Methods (including ethical
and a short title to be used as a short ‘running head’ (and
and statistical information), Results and Discussion
which should be so identi ed and should comprise up to
(including a conclusion).
is so-called
“IMRAD”
45 characters).
e rst name, middle initial and last
structure is not simply an arbitrary publication format,
name of each author should appear. If the work is to be
but rather a direct re ection of the process of scienti c
attributed to a department or institution, its full name
discovery. Long articles may require subheadings within
should be included. Any disclaimers should appear on the
some sections (especially the Results and Discussion
title page, as should the name and address of the author
sections) to clarify their content. Other types of articles,
responsible for correspondence concerning the manuscript
such as case reports, reviews, and editorials, are likely to
and the name, address and e-mail address of the author to
require other formats. Excessive use of abbreviations is
whom requests for reprints should be made (the author
not recommended. Outline statistical methods used.
should mention if he does not want his e-mail address to
Identify drugs and chemicals used by generic name (if
be published). Finally, the title page should include the
trade-marks are mentioned, manufactured name and
sources of any support for the work in the form of grants,
city should be given).
equipment, drugs, or any combination of these.
Acknowledgements
Abstracts
Acknowledgements should be made only to those
e second page should carry a structured abstract
who have made a substantial contribution to the study.
of no less than 200 words. Do not use abbreviations,
Authors are responsible for obtaining written permission
footnotes, or references.
from people acknowledged by name in case readers infer
Background & Aims
their endorsement of data and conclusions.
Describe the importance of the study and the
References
precise research objective(s) or study question(s).
References should be numbered consecutively in
Methods
the order in which they rst appear in the text.
ey
Methods should include information on the following
should be assigned Arabic numerals, which should be
aspects of study design when applicable: Design - describe
given in brackets, e.g. [12]. References should include
the basic study design, e.g. randomized controlled trial,
the names of all authors when six or fewer; when seven
cross sectional study, cohort study, case series, survey etc;
or more, list only the rst three names and add et al.
Setting - specify whether the study was conducted in a
References should also include full title and source
primary or tertiary care setting, in an ambulatory care
information. Journal names should be abbreviated as in
clinic or hospital, in the general community etc;
Index Medicus
Participants - indicate the number of study subjects and
terms_cond.html). No more than 90-100 references
how they were selected, recruited, and assigned to the
will be accepted for reviews. For Letters to the Editor,
intervention; Intervention
- report the method of
5-6 references. Avoid or keep as low as possible the use
administration and duration of the intervention.
of abstracts as references. Personal communications and
Results
unpublished work should not feature in the reference
Provide the main outcomes of the study, including
list but should appear in parentheses in the text.
con dence intervals or p values.
Unpublished work accepted for publication but not yet
Conclusion
released should be included in the reference list with the
State only conclusions that are directly supported
words “in press” in parentheses beside the name of the
by the evidence and the implications of the ndings.
journal concerned.
84
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GUIDANCE FOR DRAWING UP
a) Article:
in the metric system in terms of the International
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
System of Units (SI).
MA, Holub MC, Kovalsykz I, et al. Toward understanding
Abbreviations and symbols
the role of leptin and leptin receptor antagonism in
Use only standard abbreviations. Avoid
preclinical models of rheumatoid arthritis. Peptides
abbreviations in the title and abstract.
e full term for
2011;32:1567-74.
which an abbreviation stands should precede its rst use
b) Papers published only with DOI numbers:
in the text unless it is a standard unit of measurement.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Reprints
vascular periadventitial adipose tissue (tunica adiposa) as
Ten reprints of the published articles and two copies
an example. Cell Biol Int
2011;doi:
10.1042/
of the Journal will be supplied free of charge. If required
CBI20110422.
in a greater number, they will be available on payment
c) Book:
of the necessary cost.
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Landes Bioscience, Austin, Texas, USA. 2009.
Editorial policy
d) Book chapter:
We welcome all contributions in the eld of
[4] Jeremy L, Abe PD. Treatment Options in
medicine. We invite known personalities with expertise
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
and many published papers in a speci c eld to write
cancers in clinical practice, Springer-Verlag, London
reviews and editorials in our journal. We accept original
Limited, 2007:75-102.
papers and case reports from all countries.
e
Tables
Conexiuni Medicale/Medical Connections o ers
Each table should be assigned a Roman numeral
thorough peer review and immediate publication on
(e.g. Table III) and a brief title. Explanatory matter
acceptance.
e redactor-in-chief or one of the rst
should be placed in footnotes. Explain in footnotes all
reads the manuscripts received and in about 1-3 weeks
non-standard abbreviations that are used in each table.
decide upon their priority level: some are immediately
Identify statistical measures of variations, such as
sent to the reviewers, some are rejected without being
standard deviation and standard error of the mean. Each
sent for review and some are returned to authors with
table should be cited in the text.
suggestions for improvement before submitting them
Illustrations
to reviewers.
All graphs, photographs (on glossy paper), diagrams
will be referred to as gures and should be numbered
Peer-review procedure
consecutively in the text in Arabic numerals. If a gure
e Conexiuni Medicale/Medical Connections
has been published before, the original source must be
promotes evaluation of all the original papers by two or
acknowledged and written permission from the
three independent reviewers, of whom two are
copyright holder for both print and electronic formats
international personalities.
e peer-review process is
should be submitted with the material. Figures may be
essential for ensuring the quality of the scienti c
reduced, cropped or deleted at the discretion of the
information disseminated.
e reviewers are asked to
Editor.
evaluate the manuscript by applying the same standards
Legends for illustrations
as for the international journals.
e reviewers send
Captions should have an Arabic numeral
their comments to the Editor. e Editor will inform
corresponding to the illustration to which it refers with
the authors about the suggestions made by the referee
a title above and explanatory notes below it. Internal
and ask them to answer the questions and make the
scales should be explained and staining methods for
required corrections. is information is provided up to
photomicrographs should be identi ed.
three months from the date they submitted the paper to
Units of measurement
the journal. e revised manuscript should be sent in no
Measurements of length, height, weight, and
more than one month to the Editor. When the Editor
volume should be reported in metric units
(meter,
receives the corrected version with all changes marked,
kilogram, or litre) or their decimal multiples.
accompanied by a letter with a point-by-point reply to
Temperatures should be given in degrees Celsius. Blood
the reviewers’ comments, he sends those back to the
pressures should be given in mmHg. All hematological
same reviewer, who makes the nal recommendation for
and clinical chemistry measurements should be reported
acceptance or rejection of the manuscript.
85
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Notice to subscribers
inside front or inside back cover: Euro 350 1 issue, 1400
e annual subscription rates for 2014: 80 RON
4 issues. Full colour page ouside back cover: Euro 400 1
individual, 160 RON institutional. Foreing subscribers:
issue, 1600 4 issues. Bank account: Colegiul Medicilor
75
$ individual, 150
$ institutional. Additional postage:
Satu Mare, CUI 9839430, Banca Transilvania, branch
surface mail 20
$, for overseas air mail 40
$. Bank
Agen ia Golescu Satu Mare, IBAN: RO38 BTRL 0310
account: Colegiul Medicilor Satu Mare, CUI 9839430,
1202 K392 62XX (RON) IBAN: RO62 BTRL 0310
Banca Transilvania, branch Agen ia Golescu Satu Mare,
2202 K392 62XX (USD) Swift: BTRLRO22.
IBAN: RO38 BTRL 0310 1202 K392 62XX (RON)
IBAN: RO62 BTRL 0310 2202 K392 62XX (USD)
© Copyright Conexiuni Medicale/Medical
Swift: BTRLRO22. Orders should be sent to the
Connections, Satu Mare, 2014
Editorial O ce, Eroilor Revolu iei Pl. no.23-440055
No part of this publication may be reproduced,
Satu Mare, Romania. Tel./Fax:
+40-261-710456 or
stored in a retrieval system or transmitted in any form or
+40-361-408164, or by e-mail: colmedsm@gmail.com.
by any means without prior permission in writing of
Conexiuni
Medicale/Medical
Connections.
Notice to advertisers
Permission is not however required to copy abstracts of
Applications for advertisement space and for rates
papers or of articles on condition that a full reference to
should be addressed to the Editorial O ce of Conexiuni
the source is shown. Correspondence regarding
Medicale/Medical Connections.
2014 advertising
permission to reprint all or part of any article
rates are Euro 200 full (A4) colour page, 1 issue, and
published in this journal should be addressed to the
Euro 800 full colour page, 4 issues. Full colour page on
Editor, e-mail: colmedsm@gmail.com
86
EDITORIAL
A XI-a edi ie a Zilelor Medicale Sătmărene,
apoi două lucrări sus inute de dr. Levai Lehar: „Accident
organizată de Colegiul Medicilor Satu Mare şi Asocia ia
de muncă cu început tragic dar sfârșit fericit”, având ca și
Medicilor de Familie Satu Mare, în parteneriat cu
autori pe dr. Levai Lehar, dr. Pal Bagosi, dr. Carmen
Centrul Medical Rabin, a liat la Facultatea de Medicină
Caprar, dr. Marta Csik Maticu, dr. Olimpia Ster, dr.
Sakler, Universitatea Tel Aviv (Israel), Universitatea Titu
Irina Csutak, dr. N. Feraru, Sec ia Oftalmologie, Spital
Maiorescu Bucureşti, Facultatea de Medicină şi
Jude ean de Urgen ă Satu Mare și „Chirurgia refractivă
Medicină Dentară, Universitatea de Vest Vasile Goldiş
pentru reducerea dioptriilor”, autori: dr. Levai Lehar, dr.
Arad, s-a desfăşurat între
2-4 octombrie
2014.
Orsolya Dohi, dr. D. Aracs, dr. Angela Malachi, dr.
Președintele Comitetului Știin i c, ca în ecare an, a
Livia Olah, Sec ia Oftalmologie, Spital Jude ean de
fost d-na Prof. Univ. Dr. Rumelia Koren de la
Urgen ă Satu Mare. Dr. Cristina Maria Andrei, medic
Universitatea din Tel Aviv. Invita i speciali au fost: Acad.
specialist chirurgie vasculară, Spitalul Jude ean de
Prof. Univ. as. Dr. Virgil Enătescu, dr Ileana Filipescu,
Urgen ă Satu Mare a prezentat lucrările: „Importan a
Clinica de Reumatologie Cluj Napoca.
Compartimentului de chirurgie vasculară în cadrul SJU
Prima zi, joi, 2 octombrie a fost deschisă de către
Satu-Mare” și
„By-pass infrapopliteal în salvarea
preşedintele Colegiului Medicilor Satu Mare în prezen a
membrului inferior ischemic (caz clinic)”, a doua lucrare
reprezentan iilor institu iilor statului şi asocia iilor
având ca și coautor pe dr. Filip Dan, Spitalul Jude ean
profesionale: prefectul jude ului, dr. Eugeniu Avram,
de Urgen ă Baia Mare, Sec ia Cardiologie
primarul municipiului Satu Mare, dr. Dorel Coica,
interven ională. După pauză, lucrările au fost reluate
preşedintele Colegiului Medicilor Dentişti din Satu
prin prezentarea dr. Stelian Pop, medic primar oncologie
Mare, dr. Flaviu Simu, prorectorului Universită ii de
și hematologie:
„Tratamentul începe cu anatomia
Vest Vasile Goldiș, prof. univ. dr. Gavrilă Ardelean,
patologică; de la Simptom la Sistem, pentru calitatea
managerul Spitalului Jude ean de Urgen ă Satu Mare
actului medical”. În continuare au fost prezentate de
Erika Venemozer, președintelui Casei de Asigurări Satu
către dr. Bogdan Feciche:
„Cistectomie radicală cu
Mare ec. Georgeta Pop, directorului executiv al Direc iei
neovezică ileală. Experien a ini ială”, autori: dr. Bogdan
Sanitare a jude ului Satu Mare, dr. Dorina Dragoș
Feciche, dr. Dumitru Fanea, dr. Lilian Gorbatai, dr.
Guran. To i reprezentan ii institu iilor au exprimat
Cristian Rusu, dr. Neli Moroșanu, dr. Vitalie Moroşanu,
cuvinte de sprijin şi apreciere fa ă de lumea medicală
dr. Roxana Rugea, dr. Roxana Oltean, dr. Florian Vereș
sătmăreană.
și
„Prostatectomia radicală retropubică”, autori: dr.
Lucrările ştiin i ce au debutat cu sus inerea
Bogdan Feciche, dr. Cristian Rusu, dr. Nicolae
conferin ei
„ yroid Gland Involvement in Advanced
Salageanu, dr. Lilian Gorbatai, dr. Florian Vereș, dr.
Laryngeal Cancer - Afectarea glandei tiroide în cancerul
Vitalie Moroșanu, dr. Neli Moroșanu, dr. Roxana
laringian avansat” autori: dr. Ohad Hilly, dr. Lea Rath-
Rugea, dr. Nicolae Braniște, dr. Aurel Lupșa. Dr.
Wolfson, dr. Raanan Raz, dr. Yona Vaisbuch, dr. Yulia
Cristian Rusu a prezentat lucrările:
„Ureteroscopia
Strenov, dr. Karl Segal, dr. Jacob Shvero, dr. Rumelia
retrogradă-experien a Sec iei de Urologie a Spitalului
Koren de la Universitatea Tel Aviv, prezentată de către
Jude ean de Urgen ă Satu Mare” având ca autori pe dr.
Prof. Univ. Dr. Rumelia Koren. Au urmat: „Boala de
Cristian Rusu, dr. Bogdan Feciche, dr. Lilian Gorbatai,
re ux în patologia in amatorie cronică laringiană” autori:
dr. Nicolae Salageanu, dr. Nicolae Braniște, dr. Traianela
dr. Cornean Corina Iulia, medic rezident an I ORL, dr.
Ionescu, dr. Aurel Lupșa, dr. Neli Moroșanu, dr. Vitalie
Cornean Corina, medic primar ORL, Spitalul Jude ean
Moroșanu, dr. Roxana Rugea și
„Nefrectomia și
de Urgen ă Satu Mare, sus inută de dr. Cornean Corina,
nefroureterectomia laparoscopică-experien a colectivului
87
EDITORIAL
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
sătmărean”, autori: dr. Cristian Rusu, dr. Bogdan
apari ie”, având ca și autori pe dr. Călin Bumbulu și dr.
Feciche, dr. Lilian Gorbatai, dr. Nicolae Salageanu, dr.
Vasile Blaga. După pauză a urmat
„Cuanti carea
Tiberiu Botezan, dr. Florian Vereș, dr. Alexandru
e cacită ii terapiei biologice administrate pacien ilor cu
Vasvari, dr. Nicolae Braniște, dr. Traianela Ionescu, dr.
poliartrită reumatoidă activă” a autorilor dr. Ileana
Aurel Lupșa, dr. Neli Moroșanu, dr. Vitalie Moroșanu,
Filipescu, dr. Maria Deac, dr. Simona Rednic de la
dr. Roxana Rugea. „Evolu ia însemnărilor și documentelor
Clinica Reumatologică, Universitatea de Medicină şi
medicale. Context istoric” având ca autori pe dr. Orsolya
Farmacie „Iuliu Ha ieganu”, Cluj-Napoca, sus inută de
Horber şi dr. Karoly Zilahi, medici primari medicina
dr. Ileana Filipescu. În continuare dr Rumelia Koren a
familiei, a fost prezentată de dr. Orsolya Horber. A
prezentat conferin a
„Rolul celulelor dendritice în
urmat „Situa ia tratamentului infarctului miocardic cu
carcinomul papilar tiroidian” a autorilor dr. Rumelia
supradenivelare de segment ST (STEMI) în Satu Mare, în
Koren, dr. Ohad Hilly, dr. Lea Rath-Wolfson de la
ultimii 10 ani” al autorilor dr. Ladislau Kiss, dr. Alina
Universitatea din Tel Aviv. Au urmat prezentările sec iei
Roatiş, dr. Loredana Vinkler, dr. Ioana unaş, dr.
de ginecologie a Spitalului Jude ean Satu Mare: „TBC-
Melinda Kurtinecz, dr. Carmen Şimon, dr. Victor
ul în lăuzie” a autorilor dr. Viorica Varodi, dr. Gra ian
Orban, Sec ia Cardiologie, Spitalul Jude ean de Urgen ă
Tudor u uraș, dr. Cornel Căpitan, dr. Liviu Ardelean,
Satu Mare, prezentată de dr. Alina Roatiș. Conferin a
dr. Mircea Dragoș, dr. Vasile Matiz, dr. Ștefan Pop, dr.
„Expresia metaloproteinazelor 1 matriciale (MMPs-1) în
Carmen Derșidan, dr. Bogdan Fărcaș, dr. Manuela
carcinomul tiroidian bine diferen iat” sus inută de dr
Heim, dr. Radu Lucian Costin, dr. Anca Dascalescu-
Rumelia Koren a avut ca autori pe: dr. Aviram Mizrachi,
Bogdan, sus inută de dr Viorica Varodi și „Prezentare de
dr. Lea Rath-Wolfson, dr. Tuvia Hadar, dr. Eitan Yaniv,
caz: sarcina extrauterină-hernia internă”, autori dr.
dr. Sara Morgenstern, dr. Jacob Shvero, dr. Rumelia
Gra ian Tudor u uraș, dr. Viorica Varodi, dr. Cornel
Koren de la Universitatea din Tel Aviv. Prima zi a
Căpitan, dr. Liviu Ardelean, dr. Mircea Dragoș, dr.
lucrărilor a fost încheiată de „Medicul func ionar public.
Vasile Matiz, dr. Ștefan Pop, dr. Carmen Derșidan, dr.
O viziune politică sau politicianistă?” prezentată de dr.
Bogdan Fărcaș, dr. Manuela Heim, dr. Radu Lucian
Călin Bumbulu , având ca autori pe dr. Călin Bumbulu ,
Costin, dr. Anca Dăscălescu-Bogdan, dr. Vitalie
medic primar medicina familiei, dr. Alina Negru, medic
Morosanu, dr. Bogdan unas, precum și „Histeroscopia
primar medicina familiei, dr. Nicolae Sebastian Balaj,
diagnostică și terapeutică”, autori dr. Anca Dăscălescu-
medic specialist medicina familiei, dr. Vasile Blaga,
Bogdan, dr. Viorica Varodi, dr. Cornel Căpitan, dr.
medic specialist medicina familiei.
Liviu Ardelean, dr. Mircea Dragoș, dr. Vasile Matiz, dr.
Subliniem valoarea lucrărilor sus inute în cadrul
Ștefan Pop, dr. Carmen Derșidan, dr. Bogdan Fărcaș, dr.
Zilelor Medicale Sătmărene, una din prezentările dr
Manuela Heim, dr. Radu Lucian Costin, ultimele două
Levai Lehar, „Accident de muncă cu început tragic dar
lucrări ind prezentate de dr. Anca Dăscălescu-Bogdan.
sfârșit fericit”, ob inând ulterior premiul I la Conferin a
Două lucrări: „Ligatura variceală endoscopică- interven ie
Na ională de Oftalmologie.
salvatoare de via ă” și
„Extragerea de corpi străini
A doua zi a debutat prin lucrările:
„Pro laxia
esofagieni- interven ie endoscopică de urgen ă” l-au avut ca
borreliozei” și
„Căpușele” sus inute de dr. Margareta
autor pe dr. Marian Bogdan Zota, medic primar
Fulop, medic primar boli infec ioase, Spitalul Jude ean
gastroenterologie, Spitalul Jude ean de Urgen ă Satu
de Urgen ă Satu Mare. Lucrările au continuat cu
Mare. Ziua a doua a fost încheiată de dr. Călin Bumbulu
„Tratamentul în trepte al durerii” prezentată de dr.
cu „Migra ia medicilor din România”.
Loredana Aracs Tamas având ca și autori pe dr. Loredana
Ultima zi a manifestării sătmărene a cuprins două
Aracs Tamas, dr. Stelian Pop, dr. Bușilă Emilian, dr.
sec iuni: cea de Istorie medicală și cea de Medicină și
Susana Szentesi, sec ia oncologie medicală a Spitalului
artă. Istoria medicală a devenit deja o tradi ie ca și
Jude ean de Urgen ă Satu Mare. Au urmat două lucrări
sec iune în cadrul Zilelor Medicale Sătmărene,
„Reconstruc ia func ională a defectelor postexcizionale de
cuprinzând:
„Două comunicări privind activitatea
pleoapă superioară și inferioară cu lambouri musculare din
doctorului Lüko Bela” a autorilor dr. Alina Negru, dr.
vecinătate”, și
„Reconstruc ia uretrală în
2 timpi în
Călin Bumbulu , dr. Sebastian Balaj, dr. Vasile Blaga,
hipospadiasul penian folosind mucosa bucală și lambouri
„Istoria institu iei spitaliceşti din Tăşnad” având ca autori
vascularizate
ale
dartosului
penian.
Corec ia
dr. Zoltan Vass, Otto dr. Schmidt, „Istorii medicale în
pseudo stulei”, ale dr. Marius Dinu Roatiş, medic primar
memoriile Reginei Maria a României, vol II” cu autorii:
chirurgie plastică, Spitalul Jude ean de Urgen ă Satu
dr. Călin Bumbulu , stud. Andrei Bumbulu , Prof. Dr.
Mare. Dr. Călin Bumbulu a prezentat „Revista Medical
Rumelia Koren. Între sec iuni, dr Rumelia Koren
Connections/Conexiuni Medicale, un bilan la 9 ani de
împreună cu dr Călin Bumbulu au sus inut conferin a
88
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
EDITORIAL
„Îndrumar pentru redactarea unei lucrări ştiin i ce”. A
permanentă a Spitalului Beilinson, Petah Tikva, Israel”
urmat sec iunea de Medicină și artă cu
„Sindromul
având ca autori pe Prof. Univ. Dr. Rumelia Koren, și dr.
Marfan în pictură„ având ca autori: dr. Călin Bumbulu ,
Călin Bumbulu .
dr. Alina Negru, Prof. Dr. Rumelia Koren, „Sindromul
Auditoriul a desemnat prin vot câştigătorii celor
Langdon-Down în pictură” autori dr. Alina Negru, dr.
cinci Diplome de Excelen ă: dr. Viorica Varodi, dr.
Călin Bumbulu , Prof. Dr. Rumelia Koren,
Marius Roatiș, dr. Marian Bogdan Zota, dr. Levai Lehar,
„Reprezentarea sechelelor poliomielitei în artă” autori Prof.
dr. Margareta Fulop.
Dr. Rumelia Koren, dr. Alina Negru, dr. Călin
Edi ia a XI-a a Zilelor Medicale Sătmărene a
Bumbulu , „Picturi reprezentând un caz de obezitate din
prezentat 40 de lucrări a celor 90 de autori, în cele trei
secolul al XVII-lea, datorat probabil sindromului Prader-
zile participând
305 medici înregistra i, discu iile
Willi” autori dr. Călin Bumbulu , dr. Alina Negru, Prof.
prilejuite ind intense în special în cursul zilei a doua,
Dr. Rumelia Koren, „Cabinetul de artă și curiozită i de la
implicând probleme de ordin știin i c, dar și de
castelul Ambras, Austria” autori Prof. Dr. Rumelia Koren,
organizare administrativă a unor sec ii din Spitalul
dr. Călin Bumbulu , stud. Andrei Bumbulu , dr. Alina
Jude ean Satu Mare. Men ionăm și di cultă ile create
Negru, „Imaginează- i toate imaginile prinzând via ă” al
de închiderea aeroportului Satu Mare, chiar în perioada
autorilor dr. Gabrieli Selma, dr. Benzaquen Oshra, de la
manifestării, împiedicând asfel participarea colegilor din
Departamentul de Imagistică, Spitalul Hasharon,
București și a celor din străinătate.
Centrul Medical Rabin, Petah Tikva, Facultatea de
Sperăm că următoarea edi ie, a XII-a, care va avea
Medicină Sackler a liată Universită ii din Tel-Aviv,
loc în 2015, în prima săptamână a lunii octombrie, se va
Israel. Sec iunea a fost încheiată de lucrarea „Expozi ia
desfășura sub auspicii și mai bune.
editor şef adjunct: dr. Bumbulu Călin
89
Medical Connections/Conexiuni Medicale
Declarația de conflict de interese
Medical Connections/Conexiuni Medicale (Med Con) solicită tuturor autorilor şi recenzorilor să declare
orice con ict de interese care ar putea interveni în contribu iile lor.
Con ictul de interese pentru un anumit manuscris există atunci când un participant în procesul de
recenzie inter pares (peer review) şi de publicare - autor, referent, sau editor - are legături cu activită i care
l-ar putea in uen a necorespunzător pe el sau judecata lui, indiferent dacă aceasta este sau nu afectată.
Rela iile nanciare cu industria medicală, de exemplu prin muncă salarială, consultan ă, de inere de
ac iuni, onorarii, testimoniale ca şi expert, e direct, e prin intermediul familiei, sunt de obicei considerate
a cele mai importante con icte de interese. Cu toate acestea, pot apărea con icte din alte motive, cum ar
rela iile personale, concuren a academică şi implicarea intelectuală.
Încrederea publicului în procesul de revizuire inter pares şi credibilitatea articolelor publicate depinde
în parte de cât de bine este administrat posibilul con ict de interese în timpul redactării, recenziei inter
pares şi a luării deciziilor editoriale. Părtinirea poate de multe ori identi cată şi eliminată prin aten ia
crescută asupra metodelor ştiin i ce şi concluziilor lucrării. Rela iile nanciare şi efectele lor sunt mai uşor
de identi cat decât alte con icte de interese. Participan ii la peer review şi în procesul de publicare trebuie
să-şi dezvăluie posibilele con ictele de interese, iar informa iile trebuie să e puse la dispozi ie, astfel încât
şi al ii să poată aprecia aceste efecte pentru ei înşişi.
Autori: atunci când trimit un manuscris sau o scrisoare, autorii sunt responsabili pentru recunoaşterea
şi divulgarea con ictelor nanciare şi altor con icte de interese care ar putea să le in uen eze activitatea. Ei
trebuie să recunoască în manuscris orice sprijin nanciar pentru activitate, precum şi orice alte legături
nanciare sau personale în munca lor.
Recenzorii: evaluatorii externi inter pares trebuie să dezvăluie editorilor orice con icte de interese care
le-ar putea părtini opiniile asupra manuscrisului şi ar trebui să se recuze de la recenzia anumitor manuscrise
în cazul în care cred că este oportun. Editorii trebuie să e conştien i de posibilele con icte de interese ale
recenzorilor în interpretarea recenziilor şi trebuie să judece pentru ei dacă recenzorul ar trebui să e recuzat.
Recenzorii nu trebuie să utilizeze informa iile în munca lor, înainte de publicare, pentru a-şi promova
propriile interese.
Titlul manuscrisului: ________________________________________________________
Declar că nu există con ict de interese
Declar că există următoarele con icte de interese poten iale:
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________________________________________________
_________________________________
_________________________________
Nume
Semnătura/Data
Vă rugăm trimite i acest formular semnat pe fax sau mail la sediul editorului Med Con.
Fax: +40-261-710456
Email: colmedsm@gmail.com
ORIGINAL ARTICLES
EVALUAREA PRECONDIȚIONĂRII ISCHEMICE MIOCARDICE
CUANTIFICÂND ACTIVITATEA ELECTRICĂ ȘI MECANICĂ POST
ISCHEMICĂ FOLOSIND CORDURI DE ȘOBOLAN EX VIVO
Mihai Mărginean1,4, Alina Ardelean-Maghiar2,5, Ovidiu Simion Cotoi3, Gheorghe Bărbat1, Marcel Perian1
Departamentele de 1Fiziologie, 2Medicină de Laborator, 3Biologie Celulară și Moleculară, UMF Târgu-Mureș și 4Sec ia
de Anestezie și Terapie Intensivă și 5Laborator Clinic, Spitalul Militar de Urgen ă „Dr. Constantin Papilian”, Cluj-
Napoca, România
Adresa pentru coresponden ă:
Mărginean Mihai
Str. Ana Aslan nr. 18, Cluj-Napoca, Cluj, România
Tel: +4 0754700271
E-mail: marginean.m@gmail.com
Primit: 23.07.2014
Acceptat: 15.09.2014
Med Con October 2014, Vol 9, No 3, 91-97
Rezumat
au fost monitorizate frecven a cardiacă, ECG într-o
singură deriva ie și presiunea din ventricolul stâng. La
Introducere:
După descoperirea
efectului
nalul protocolului experimental atriile au fost
precondi ionant al ischemiei și efectul său protector
îndepărtate, iar miocardul ventricular a fost submersat
împotriva unei agresiuni ischemice ulterioare, cercetătorii
în solu ie de Formaldehidă. Ulterior s-au practicat studii
au încercat să în eleagă mai bine căile moleculare
histologice folosind colora ia Hematoxilină&Eozină.
implicate. Pe parcursul acestui experiment am încercat să
Rezultate: În ceea ce privește persisten a activită ii
ob inem date suplimentare despre modul cum activitatea
mecanice nu am găsit nicio diferen ă semni cativă între
mecanică și electrică a cordului ex-vivo este in uen ată de
cele două grupuri (p=0,08). Perioada în care cordurile și-
un singur ciclu de ischemie/reperfuzie.
au men inut o activitate electrică măsurabilă după
Material și metode: Am folosit 30 de șobolani
agresiunea ischemică prelungită a fost diferită semni cativ
Wistar adul i care au fost atribui i aleator către două
statistic (p=0,01). La nalul perioadei de ischemie și după
grupuri: grupul cu precondi ionare ischemică
(IPC,
restabilirea perfuziei retrograde nu am înregistrat activitate
n=15) și grupul control (C, n=15). După ob inerea
mecanică la niciun preparat din cele două grupuri studiate,
anesteziei
(cu Ketamină și Xilazină) și anticoagulării
însă 11 (din 15 preparate) din grupul IPC și-au recăpătat
e ciente (cu Heparină nefrac ionată) cordurile au fost
activitatea electrică pentru încă aproximativ 25 minute.
excizate și perfuzate retrograd folosind un dispozitiv
Concluzii: Precondi ionarea cordurilor de șobolan ex-
Langendor . După o perioadă de stabilizare, toate
vivo folosind un singur ciclu de ischemie/reperfuzie are ca
cordurile din grupul IPC au fost supuse unui protocol
rezultat o activitate electrică mai persistentă pe perioada
de precondi ionare ce constă dintr-un ciclu de 5 minute
unei agresiuni ischemice ulterioare comparativ cu cordurile
de ischemie, urmat de 5 minute de reperfuzie înaintea
fără precondi ionare, în timp ce activitatea mecanică nu
unei perioade de
30 minute de ischemie sus inută.
pare să e in uen ată de acest protocol de precondi ionare.
Grupul de control a fost supus doar unei perioade de 30
Cuvinte cheie: precondi ionare ischemică, șobolan
de minute de ischemie. Pe toată durata experimentului Wistar, infarct miocardic
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
91
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Introducere
lor kinaza glicogen-sintetaza
3b (glycogen syntethase
kinase 3b; GSK-3b) care duce la inhibarea deschiderii
În 1986 Murry și colab. [1] au observat că episoade
porului mitocondrial de permeabilitate a tranzi iei
scurte de ischemie miocardică au un efect neașteptat și
(mitochondrial permeability transition pore; mPTP)
paradoxal de reducere a dimensiunii infarctului cauzat
[10]. Calea SAFE (survivor activating factor enhancement)
de ocluzia arterei coronare circum exe cu până la 75%.
care implică factorul de necroză tumorală (TNFα) și
Ei au folosit patru cicluri de ischemie/reperfuzie (I/R)
factorul transmi ător de semnal și activator al transcrip iei
de câte 5 minute ecare. Această capacitate a miocardului
3 (signal transducer and activator of transcription-3;
de a tolera o injurie ischemică sus inută după episoade
STAT-3) [11] duce de asemenea la inhibarea deschiderii
scurte de I/R a fost denumită pre-condi ionare ischemică
mPTP. Așadar, se poate a rma că mPTP este principalul
(IPC). Acest fenomen cardio-protector a fost con rmat
efector al pre-condi ionarii [12]. Deschiderea acestui por
ulterior la toate speciile animale studiate.
oprește produc ia de ATP, induce balonarea mitocondrială
În timpul IPC, efectul protector are două etape.
și creează premisele rupturii membranare [13]. Activarea
Prima fază începe imediat după declanșarea pre-
altor kinaze cum este protein-kinaza C [14] și protein-
condi ionării de către un trigger și durează
2-4 ore.
kinaza G [15] este responsabilă de activarea canalelor
Această fază a fost numită pre-condi ionare ischemică
mitocondriale de potasiu ATP-dependente (mKATP), care
clasică. O fază tardivă a efectului protector, denumită a
sunt de asemeni efectori ai IPC [16,17].
doua fereastră de protec ie (SWOP) începe după 12-24
Aceste căi de semnalizare intracelulară complexe
de ore și durează 2-3 zile [2]. Pre-condi ionarea ischemică
ridică o serie de întrebări care au rămas neclari cate chiar
implică mai mul i factori care de regulă sunt împăr i i în
și după mai multe decenii de cercetare în acest domeniu.
trei categorii: trigger-i, mediatori și efectori, însă căile de
Obiectivul nostru a fost acela de a oferi date
transmitere a semnalelor între aceștia sunt complexe și
suplimentare în legătură cu intervalul de timp scurs
incomplet în elese. Episoadele scurte de ischemie
până la pierderea completă a activită ii electrice și
determină eliberarea unor factori ini iatori cum sunt
mecanice după o leziune ischemică la nivelul esutului
adenozina, bradikinina sau endor nele [3,4] (Figura 1).
miocardic pre-condi ionat cu un singur ciclu de I/R.
În timpul primei faze acești ini iatori se leagă de receptori
speci ci cupla i cu proteina G, ceea ce are ca rezultat
Material și metodă
transmiterea semnalului. Au fost identi cate două căi de
transmitere a semnalului. Una dintre acestea, kinaza de
Acest experiment a fost realizat în cadrul
salvare indusă de reperfuzie (Reperfusion-Induced Salvage
Compartimentului de Fiziologie Cardiovasculară al
Kinase; RISK) [5] include fosfatidil inozitol-3 kinaza
Catedrei de Fiziologie, Universitatea de Medicină și
(PI3-kinase) [6,7] protein-kinaza Akt [8] și kinaza ½
Farmacie Tîrgu-Mureș.
extracelulară reglată de semnal
(extracellular signal-
Protocolul experimental a fost conceput astfel încât
regulated kinase ½) [9]. Aceste kinaze activează la rândul
să se supună directivelor Uniunii Europene cu privire la
protec ia animalelor folosite în scopuri știin i ce.
Am folosit 30 de șobolani Wistar adul i (cu vârste
cuprinse între 5 și 8 luni) adăposti i în condi ii controlate
de temperatură, hrăni i ad libitum cu alimenta ie
standard pentru rozătoare și cu o masă corporală între
250 g și 350 g. Aceștia au fost randomiza i în două
grupuri: cel cu pre-condi ionare ischemică (IPC, n=15)
și grupul de control
(C, n=15). Animalele au fost
anesteziate folosind Ketamină 100 µg/kg și Xilazină 10
µg/kg administrate intraperitoneal [18]. După induc ia
anestezică a fost realizată o incizie medio-abdominală de
2-3 cm, con inutul intraperitoneal a fost luxat și s-a
exprimat vena renală stângă. Am administrat 50 UI/100g
Heparină sodică prin punc ionarea directă a venei renale
[19], iar după ob inerea unei anticoagulări e ciente
(con rmată prin sângerare difuză spontană la nivelul
inciziei cutanate), incizia chirurgicală ini ială a fost
Figura 1. Căile de semnalizare ale pre-
condi ionării ischemice (IPC)
extinsă subcostal bilateral pentru a avea un bun acces la
92
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
mușchiul diafragm. Acesta a fost incizat descoperind
Activitatea electrică a fost înregistrată folosind doi
astfel cavitatea toracică, cu vizualizarea cordului. Sacul
electrozi dintr-un aranjament de cinci dispuși în jurul
pericardic a fost incizat, iar cordul a fost excizat la nivelul
cordului. După canularea aortei și pozi ionarea corectă a
aortei descendente imediat sub arcul aortic și introdus în
sondei de presiune în interiorul ventricolului stâng,
solu ie Krebs-Henseleit
(K-H) la
4°C
[20]. Solu ia
întregul montaj capătă o pozi ie xă. Pentru înregistrarea
nutritivă K-H a fost pregătită extemporaneu, înainte de
activită ii electrice am ales un electrod din vecinătatea
ecare sesiune experimentală, după o re etă standard
atriului drept și al doilea lângă atriul stâng, astfel că s-a
[19,21,22] și folosită nu mai mult de 24 ore. Timpul de
ob inut o deriva ie similară DI (Figura 2). Dispozitivul
la incizia mușchiului diafragm
(moment în care
folosit pentru înregistrarea ECG ne permite alegerea
respira iile spontane devin ine ciente) până la montarea
diferitelor combina ii de electrozi în func ie de
cordului în dispozitivul Langendor și ini ierea perfuziei
pozi ionarea nală a cordului în dispozitivul Langendor .
retrograde a fost păstrat sub 3 minute. Solu ia K-H a fost
Amplitudinea semnalului înregistrat a fost calibrată
oxigenată în permanen ă prin barbotarea unui ux
folosind un curent electric de 1 mV [23] (Figura 3).
constant de oxigen și a fost perfuzată la o presiune (75
Aplica ia folosită pentru a șarea și interpretarea
mmHg) și temperatură
(37°C) constantă. După
semnalului ECG permite și măsurători de timp. Astfel,
începerea perfuziei miocardice s-a practicat o incizie la
cunoscând perioada exactă între două unde R, am
nivelul atriului stâng, iar sonda de presiune a fost
determinat frecven a cardiacă
(FC=1000/t(msec.)x60).
avansată prin atriu, în ventricolul stâng. A urmat o
Activitatea mecanică a cordului a fost evaluată folosind
perioadă de stabilizare de 20 de minute, la sfârșitul căreia
un transductor de presiune conectat la un balon (umplut
toate cordurile incluse în studiu prezentau un ritm
sinusal stabil și o alură constantă [19]. Pentru grupul
IPC, după perioada ini ială de stabilizare, a urmat o
perioadă de 5 minute de ischemie (indusă prin oprirea
manuală a perfuziei cu solu ie K-H), urmată de 5 minute
de reperfuzie, după care 30 minute de ischemie sus inută.
Grupul de control (C) a fost supus numai perioadei de
Figura 3. Calibrarea ECG folosind un curent
ischemie de 30 minute. După aceea a urmat o perioadă
de 1mV
obligatorie de stabilizare cu durata de 40 minute, astfel
încât metaboli ii rezulta i în urma leziunii ischemice să
e spăla i pentru a evita inducerea leziunii celulare după
ce perioada de ischemie s-a încheiat. Un sumar al acestui
protocol este ilustrat în Tabelul I.
Figura 4. ECG (prima curbă) și presiunea din
VS (a doua curbă). Înregistrare din timpul
perioadei de stabilizare (minutele 0-20).
FC=178 b/min
Figura 5. Episod de brila ie ventriculară
înregistrat în cadrul grupului C în timpul
Figura 2: Pozi ionarea electrozilor CG
perioadei de ischemie sus inută
Tabel I. Protocolul utilizat
20 min
10 min
30 min
40 min
CONTROL
STABILIZATION
monitoring
ISCHAEMIA
REPERFUSION
20 min
5
5
30 min
40 min
IPC
STABILIZATION
I
R
ISCHAEMIA
REPERFUSION
minutes
10
20
30
40
50
60
70
80
90
100
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
93
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Figura 6. Frecven a cardiacă înregistrată
Figura 8. Momentul în care activitatea
în minutul 20 al protocolului de IPC
mecanică a VS încetează (media±DS),
(media±DS), p=0.8
p=0,08
Figura 7. Frecven a cardiacă înregistrată în
Figura 9. Momentul când încetează activitatea
minutul 30 al protocolului de IPC
electrică, (media±DS), p=0,01
(media±DS), p=0,49
cu apă), care a fost introdus în VS. Înregistrările de
altfel). O valoare a p sub
0,05 a fost considerată
presiune și ECG au fost a șate simultan (Figura 4).
semni cativă. Pentru managementul statistic al datelor
ECG într-o singură deriva ie și presiunea din VS au
am folosit programe disponibile comercial (GraphPad
fost înregistrate continuu până când atât activitatea
Prism ver.5.03 pentru Windows©, GraphPad Software,
electrică, cât și cea mecanică a inimii au încetat. Chiar
San Diego California USA).
dacă acest lucru s-a întâmplat la câteva minute după
începutul perioadei lungi de ischemie (minutele 30-60,
Rezultate
Tabel I), la sfârșitul acestei perioade s-a ini iat reperfuzia,
care a continuat pentru încă 40 de minute (minutele 60-
Frecven a cardiacă înregistrată în minutul 20 (vezi
100, Tabel I) [1]. În cadrul acestui experiment nu s-au
Tabelul I pentru clari care), la sfârșitul perioadei de
realizat studii de morfologie sau ritm a activită ii electrice
stabilizare, atât la subiec ii din lotul C, cât și din lotul
cardiace. Orice tip de ritm
(cu excep ia brila iei
IPC, nu a fost diferită din punct de vedere statistic
ventriculare, Figura 5) a fost considerat activitate electrică.
(p=0,83) (Figura 6).
Activitatea mecanică a fost considerată absentă atunci
Nici în minutul 30, la sfârșitul ciclului de I/R, nu am
când nu s-a mai putut observa o undă individuală de
găsit diferen e semni cative statistic (p=0,49) (Figura 7).
presiune. La sfârșitul celor 100 de minute ale protocolului,
Momentul când sonda de presiune din VS a încetat
atriile au fost excizate, iar miocardul ventricular a fost
să mai înregistreze un semnal vizibil nu a fost nici acesta
introdus în formaldehidă (solu ie 37%) pentru xare.
diferit la cele două grupuri (p=0,08). În ambele grupuri
După cel pu in 24 de ore s-a realizat un studiu histologic
activitatea mecanică a fost pierdută după aproximativ
folosind o colora ie cu Hematoxilină și Eozină.
32-33 minute (C, 1932±82 sec; IPC, 1976±83 sec) (la
Analiza statistică
2-3 minute după începerea perioadei de ischemie)
Am comparat intervalul de timp de la începutul
(Figura 8).
perioadei de ischemie sus inută de 30 minute (minutul
În ceea ce privește activitatea electrică am observat o
30, Tabel I) până la pierderea completă a activită ii
diferen ă semni cativă între cele două grupuri (p=0,01).
electrice și mecanice a cordurilor de șobolan. Rezultatele
În grupul C s-au înregistrat impulsuri electrice cardiace
au fost prezentate ca medie±DS (dacă nu este speci cat
timp de aproximativ 38 minute (C, 2332±225 sec), iar
94
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
A
B
C
Figura 10. Examinare histologică. Grupul control. Colora ie cu H&E. A. Miocard ventricular. Ischemie acută. Fibre
miocardice fragmentate, citoplasma hipereozino lică, dispari ia focală a nucleilor, Ob 4x. B. Miocard ventricular. Ischemie
acută. Focare de ischemie la nivelul mușchilor papilari, Ob 4x. C. Miocard ventricular. Ischemie acută.
Miocardiocite cu citoplasmă hipereozino lică, stria ii disipate, absen a nucleilor, Ob 10x
A
B
C
Figura 11. Examinare histologică. Grupul cu pre-condi ionare ischemică (IPC). Colora ie H&E. A. Miocard ventricular. Focare de
ischemie acută vizibile în peretele miocardic, Ob 2x. B. Miocard ventricular. Focare de ischemie acută vizibile în peretele miocardic,
Ob 4x. C. Miocard ventricular. Ischemie acută. Miocardiocite cu citoplasmă hipereozino lă, stria ii disipate, absen a nucleilor, Ob 4x.
pentru grupul cu IPC timp de aproximativ 42 minute
nicio diferen ă în ceea ce privește statusul ini ial al
(IPC, 2548±231 sec) (Figura 9).
cordurilor înainte de ini ierea protocolului de IPC. Testele
Pentru analiza statistică am folosit perioadele de
statistice au con rmat acest lucru (p=0,83) așa cum era de
timp de la începutul protocolului de IPC (Tabel I).
așteptat. Însă, chiar și după 5 minute de ischemie, nu am
După ultima perioadă ischemică (minutele 30-60),
găsit nicio diferen ă în ceea ce privește FC (Figura 7,
în momentul repornirii perfuziei retrograde, nu am mai
p=0,49). Așadar, valoarea FC ca și parametru de
înregistrat activitate mecanică ulterioară în niciunul
monitorizare va trebui augmentată în studii ulterioare
dintre grupurile studiate. 11 corduri (din 15) incluse în
prin adăugarea unor parametrii adi ionali
(cum este
grupul IPC și-au reluat activitatea electrică, care a mai
imagistica optică [24] și/sau markeri de necroză miocardică
durat încă aproximativ 25 minute (după perioada de 30
- ex: troponina cardiacă). De vreme ce nu am analizat din
minute de ischemie) (IPC, 1511±450 sec).
punct de vedere morfologic activitatea electrică a cordului,
Studiile histologice au oferit pu ine date adi ionale.
date exacte despre ritm nu sunt disponibile. Am considerat
Acestea au con rmat leziunile ischemice acute în ambele
orice fel de ritm ca ind activitate electrică, cu excep ia
grupuri și au eviden iat un grad mai mare de alterare
brila iei ventriculare (Figura 5).
tisulară pentru grupul care nu a fost pre-condi ionat (C)
Cu privire la curba de presiune ob inută din VS, nu
(Figura 10) dar cuanti carea exactă și analiza statistică
am putut realiza o analiză extensivă (cum ar măsurarea
nu au fost posibile din cauză că leziunile au fost difuze (și
ariei-de-sub-curbă, AUC), din cauza limitărilor de software.
nu focale), iar esutul ischemic alterna cu cel neafectat.
Datele noastre sugerează că în timpul unei perioade
Așadar, nu s-a putut folosi analiza de contur. Preparatele
de ischemie sus inută, activitatea electrică persistă mai
histologice din lotul IPC sunt ilustrate în Figura 11.
mult timp în grupul cu pre-condi ionare ischemică, în
timp ce activitatea mecanică nu pare să e in uen ată de
Discuții
IPC [25]. Mecanismul care stă la baza acestor observa ii
este probabil legat de diferen ele de disponibilitate și
Înregistrând frecven a cardiacă la sfârșitul perioadei
utilizare a ATP. În ambele grupuri, cantitatea de ATP
de stabilizare (Figura 6) am dorit să arătăm că nu există
generată în condi ii de ischemie este cel mai probabil
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
95
Ex-Vivo Rat Hearts
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
insu cientă pentru a sus ine activitatea mecanică, acesta
Resurselor Umane (POSDRU) cu nan are de la Fondul
ind motivul pentru care nu există o diferen ă statistică
Social European și Guvernul României cu numărul
între cele două grupuri. Pe de altă parte, de vreme ce
POSDRU/CPP107/DMI1.5/S/80641
și
pre-condi ionarea ischemică poate ajuta la o mai bună
POSDRU/159/1.5/S/133377.
conservare a nivelelor de ATP [26], rezultând niveluri
Proiect nan at prin Granturile interne de cercetare de
mai mari în cordurile cu IPC, ceea ce explică persisten a
către Universitatea de Medicină şi Farmacie din Tîrgu
activită ii electrice. Deschiderea canalelor de potasiu
Mureş, România; (CIGCS 20/11.12.2013).
dependente de ATP (IK-ATP) ca răspuns la creșterea intra-
celulară a ATP indusă de ischemie, explică accelerarea
fazei 3 a poten ialului de ac iune, fenomen observat la
Referințe
miocitele supuse pre-condi ionării ischemice. Acest
lucru scade timpul pentru in uxul de Ca2+ prin canalele
1.
Murry CE, Jennings RB, Reimer KA. Preconditioning
de tip L din timpul fazei de platou a poten ialului de
with ischemia: a delay of lethal cell injury in ischemic
ac iune, prevenind astfel supra-încărcarea apoptotică cu
myocardium. Circulation 1986;74(5):1124-36.
calciu
[27,28]. Acest fenomen explică persisten a
2.
Marber MS, Latchman DS, Walker JM, Yellon DM.
activită ii electrice observată în grupul cu IPC.
Cardiac stress protein elevation
24 hours after brief
Studiile histologice au fost limitate de posibilită ile de
ischemia or heat stress is associated with resistance to
colorare. Pentru etape ulterioare de cercetare propunem
myocardial infarction. Circulation 1993;88(3):1264-
folosirea unor indicatori redox pentru a evalua corect
72.
respira ia celulară (ex: clorură 2,3,5-trifenil-2H-tetrazoliu,
3.
Downey JM, Davis AM, Cohen M V. Signaling
TTC) și în același timp pentru a avea posibilitatea de a
pathways in ischemic preconditioning. Heart Fail Rev
măsura aria infarctizată utilizând o aplica ie software de
2007;12(3-4):181-8.
urmărire a conturului [29,30]. Așa cum am men ionat,
4.
Cohen M V, Yang X-M, Liu GS, Heusch G, Downey
aceste analize nu au fost posibile pentru acest studiu.
JM. Acetylcholine, Bradykinin, Opioids, and
O altă limitare a fost legată de drogurile anestezice
Phenylephrine,
but
not
Adenosine,
Trigger
utilizate. Există date care arată că utilizarea Ketaminei
Preconditioning by Generating Free Radicals and
poate reduce efectul pre-condi ionant ischemic mergând
Opening Mitochondrial KATP Channels. Circ Res
până la blocarea completă a acestuia [31]. Cu toate
2001;89(3):273-8.
acestea, am fost nevoi i să utilizăm acest anestezic
5.
Hausenloy DJ, Tsang A, Yellon DM. e reperfusion
deoarece nu am dispus de un înlocuitor potrivit la
injury salvage kinase pathway: a common target for both
momentul experimentului.
ischemic preconditioning and post conditioning. Trends
Pe de altă parte, pentru acest studiu am folosit un
Cardiovasc Med 2005;15(2):69-75.
singur ciclu de ischemie/reperfuzie, ceea ce contrastează cu
6.
Qin Q, Downey JM, Cohen M V. Acetylcholine but
majoritatea lucrărilor publicate până în prezent,
not adenosine triggers preconditioning through PI3-
considerând astfel că am avut o contribu ie, e ea modestă,
kinase and a tyrosine kinase. Am J Physiol Heart Circ
la creșterea calită ii informa iei existente în legătură cu
Physiol 2003;284(2):H727-34.
magnitudinea efectului unui ciclu unic de I/R.
7.
Tong H, Chen W, Steenbergen C, Murphy E. Ischemic
Preconditioning Activates Phosphatidylinositol-3-Kinase
Concluzii
Upstream of Protein Kinase C. Circ Res
2000;87(4):309-15.
Am concluzionat că pre-condi ionarea cordurilor
8.
Krieg T, Qin Q, Philipp S. Acetylcholine and
ex-vivo de șobolan folosind un singur ciclu de I/R are ca
bradykinin trigger preconditioning in the heart through
rezultat persisten a activită ii electrice pentru o durată
a pathway that includes Akt and NOS. Am J Physiol
de timp mai lungă pe perioada unei injurii ischemice
Heart Circ Physiol 2004;36688:2606-11.
sus inute și prelungite, comparativ cu cordurile fără pre-
9.
Hausenloy DJ, Tsang A, Mocanu MM, Yellon DM.
condi ionare. În același timp, activitatea mecanică a
Ischemic preconditioning protects by activating
cordului nu pare să e in uen ată de pre-condi ionarea
prosurvival kinases at reperfusion. Am J Physiol Heart
ischemică.
Circ Physiol 2005;288(2):H971-6.
10.
Juhaszova M, Zorov DB, Kim SH, et al. Glycogen
Mul umiri
synthase kinase-3beta mediates convergence of protection
Proiect co nan at din Fondul Social European prin
signaling to inhibit the mitochondrial permeability
Programul Opera ional Sectorial pentru Dezvoltarea
transition pore. J Clin Invest 2004;113(11):1535-49.
96
Mărginean et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
11.
Suleman N, Somers S, Smith R, Opie LH, Lecour
against global ischemia with Krebs-Henseleit bu er-
SC. Dual activation of STAT-3 and Akt is required
based cardioplegic solution. J Cardiothorac Surg
during the trigger phase of ischemic preconditioning.
2013;8:60.
Cardiovasc Res 2008;79(1):127-33.
21.
Gillis AM, Kulisz E, Mathison HJ. Cardiac
12.
Bousselmi R, Lebbi MA, Ferjani M. Myocardial
electrophysiological variables in blood-perfused and
ischemic conditioning: Physiological aspects and clinical
bu er-perfused isolated, working rabbit heart. Am J
applications in cardiac surgery. J Saudi Hear Assoc
Physiol Heart Circ Physiol 1996;271(2):H784-789.
2014; 26(2):93-100.
22.
Lu M, Atthe B, Mateescu G. Assessing mitochondrial
13.
Hausenloy DJ, Maddock HL, Baxter GF, Yellon DM.
respiration in isolated hearts using 17O MRS. NMR
Inhibiting mitochondrial permeability transition pore
Biomed 2012;25(6):883-9.
opening: a new paradigm for myocardial preconditioning?
23.
Perian M, Dobreanu D, Caldararu C, Sabau M. A
Cardiovasc Res 2002;55(3):534-43.
Simple ECG Recording Hardware for Langendor
14.
Liu GS, Cohen M V, Mochly-Rosen D, Downey JM.
Isolated Heart Experiments. Fiziol
- Physiol
Protein kinase C-epsilon is responsible for the protection
2012;3(38):38-40.
of preconditioning in rabbit cardiomyocytes. J Mol Cell
24.
E mov IR, Nikolski VP, Salama G. Optical Imaging of
Cardiol 1999;31(10):1937-48.
the Heart. Circ Res 2004;95(1):21-33.
15.
Costa ADT, Garlid KD, West IC, et al. Protein kinase
25.
Yellon D, Alkhulai A, Pugsley W. Preconditioning the
G transmits the cardioprotective signal from cytosol to
human myocardium. Lancet 1993;342(8866):276-7.
mitochondria. Circ Res 2005;97(4):329-36.
26.
Noma A. ATP-regulated K+ channels in cardiac muscle.
16.
Gross GJ, Auchampach J A. Blockade of ATP-sensitive
Nature 1983;305(5930):147-8.
potassium channels prevents myocardial preconditioning
27.
Cole WC, McPherson CD, Sontag D. ATP-regulated
in dogs. Circ Res 1992;70(2):223-33.
K+ channels protect the myocardium against ischemia/
17.
Pain T, Yang X-M, Critz SD, et al. Opening of
reperfusion damage. Circ Res 1991;69(3):571-81.
Mitochondrial KATP Channels Triggers the
28.
Takagawa J, Zhang Y, Wong ML, et al. Myocardial
Preconditioned State by Generating Free Radicals. Circ
infarct size measurement in the mouse chronic infarction
Res 2000;87(6):460-6.
model: comparison of area- and length-based approaches.
18.
Animal Care and Use Program. University of
J Appl Physiol 2007;102(6):2104-11.
California, Berkeley. Guidelines for Anaesthesia and
29.
Nascimento DS, Valente M, Esteves T, et al.
Analgesia in Laboratory Animals. 2012;p 1-5.
MIQuant-semi-automation of infarct size assessment in
19.
Arnaud C, Cracowski J-L, Hakim A, et al. 15-F2t-
models of cardiac ischemic injury. PLoS One
isoprostane and
5-F2t-isoprostane are not triggers of
2011;6(9):e25045.
myocardial preconditioning. Clin Exp Pharmacol
30.
Müllenheim J, Frässdorf J, Preckel B,
ämer V,
Physiol 2005;32(5-6):350-4.
Schlack W. Ketamine, but not S(+)-ketamine, blocks
20.
Minasian SM, Galagudza MM, Dmitriev Y V,
ischemic preconditioning in rabbit hearts in vivo.
Kurapeev DI, Vlasov TD. Myocardial protection
Anesthesiology 2001;94(4):630-6.
Evaluating Myocardial Ischemic Preconditioning by Quantifying Post-Ischemic Mechanical and Electrical Activity Using
97
Ex-Vivo Rat Hearts
Scrisoare de informare
Având în vedere activită ile revistei Medical Connections/Conexiuni Medicale privind recenzia şi
editarea articolului mai jos numit, efective odată cu acceptarea acestuia de către Medical Connections/
Conexiuni Medicale (la care se face referin ă în continuare ca Med Con), autorul (autorii) atribuie prin
prezenta către Med Con, reprezentan ilor legali, succesorilor şi mandata ilor ei, toate drepturile de
publicare şi ecare şi oricare drept privind articolul în întreaga lume, în orice limbă şi în orice mediu, chiar
şi ca lucrare audiovizuală, colectivă, compila ie, lucrare derivată, lucrare în comun, operă literară,
înregistrare audio, în imagini, gra că, operă de artă vizuală, program de calculator, sau orice alt mediu
existent acum sau care va deveni ulterior uzual, inclusiv drepturile de autor şi dreptul de a înregistra
dreptul de autor, precum şi dreptul de a asigura orice reînnoire, reeditare şi extinderea unor astfel de
drepturi de autor în România sau în orice ară străină. Autorul (Autorii) pot solicita permisiunea de a
reutiliza manuscrisul sau por iuni din acesta. Astfel de cereri trebuie să e în scris, iar permisiunea dată de
Med Con nu va refuzată în mod nejusti cat. Autorul (Autorii) desemnează Med Con ca reprezentant
legal al acestuia (acestora) pentru a întocmi orice documente pe care Med Con le consideră necesare
pentru a înregistra oricare dintre aceste garan ii la o ciul de copyright românesc sau din alte ări. Autorul
(Autorii) garantează de asemenea către Med Con că articolul este lucrarea originală a autorului (autorilor),
cu excep ia materialelor provenite din domeniul public, iar fragmente din alte lucrări pot incluse doar cu
acordul prealabil scris al titularilor drepturilor de autor, că articolul nu a fost publicat anterior, nu a fost
prezentat, sau acceptat pentru publicare în altă parte, că autorul (autorii) nu au nicio rela ie, nanciară sau
de altă natură, cu orice producător sau distribuitor de produse evaluate în această lucrare, sau, dimpotrivă,
orice astfel de rela ie a fost dezvăluită într-o notă de subsol la articol, sau că această cerin ă este irelevantă
pentru lucrare.
Titlul manuscrisului: ________________________________________________________
Nume:
Semnătură/Data:
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
___________________________________
Vă rugăm trimite i pe fax +40-261-710456 această scrisoare la sediul editorului Med Con.
ORIGINAL ARTICLES
EVALUAREA HISTOPATOLOGICĂ COMPARATIVĂ A PROCESELOR
DE OSTEOINTEGRARE A IMPLANTURILOR DE TITAN ȘI ZIRCONIU
ÎN OSUL FEMURAL LA IEPURE
Bogdan A Bumbu, Bogdan Uivărășeanu, Adrian G Bumbu, Traian T Maghiar
Facultatea de Medicină și Farmacie, Universitatea din Oradea
Adresa pentru coresponden ă:
Dr. Bogdan Bumbu
Email: bogdanbumbu@yahoo.com
Primit: 02.09.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 99-104
Rezumat
speciale pentru ca el să e tolerat de organism, chiar
dacă acesta îl percepe ca pe un corp străin. În acelaşi
Implanturi de titan şi zirconiu au fost inserate în
timp, implantul trebuie să permită proliferarea
osul femural la iepuri în vârstă de 7 luni, crescu i în
corespunzătoare a esuturilor reparatorii în jurul său,
biobază unde au bene ciat de condi ii corespunzătoare
până la încorporarea lui totală în esutul dur
(os).
şi controlate. După trei săptămâni, iepurii au fost
Încorporarea trebuie să e atât de bine făcută încât să-i
sacri ca i şi s-a recoltat femurul pentru efectuare de
asigure implantului stabilitate/rezisten ă la solicitările
investiga ii histopatologice. Examenul microscopic a
mecanice (presiuni, trac iuni, etc.) la care urmează să e
eviden iat procese de osteointegrare a ate în plin proces
supusă zona în care este el inserat. Pentru ca organismul
de derulare, dar încă departe de a
nalizate. Osul nou
să-l tolereze cât mai bine şi să-l încorporeze cât mai solid
format îmbracă intim implantul pe o anumită suprafa ă
în esutul dur, materialul implantului trebuie să aibă o
şi are la acest moment al experimentului tendin ă clară
serie de proprietă i speci ce. Aceste proprietă i se referă
de extindere. Deşi nu există diferen e semni cative în
în special la aspecte de biocompatibilitate, construc ie
privin a derulării proceselor de osteointegrare între cele
implant şi biomecanică [1].
două tipuri de implanturi, totuşi la cel de zirconiu ele
Biocompatibilitatea se referă la rela iile şi reac iile ce
par ceva mai avansate.
se stabilesc între biomateriale şi esuturile gazdă. În
Cuvinte cheie: osteointegrare, os femural, titan,
cazul esuturilor dure, biocompatibilitatea se manifestă
zirconiu
la interfa a dintre implant şi osul care proliferează în
jurul lui. Niciun material heterolog nu va acceptat în
Introducere
totalitate de organism, deoarece el este recunoscut de
sistemul imun ca ind non self. El reprezintă pentru
Utilizarea biomaterialelor pentru implantare în
organism un intrus, care oricât ar persista în organism
esuturile dure capătă o amploare tot mai mare odată cu
nu va niciodată considerat structură proprie. Este
trecerea timpului. Fiind materiale heteroloage, este
foarte importantă însă reac ia organismului fa ă de acest
foarte important ca înainte de utilizarea oricărui material
corp străin şi în func ie de calită ile materialului din care
de implant, el să e foarte minu ios testat din mai multe
este confec ionat implantul, organismul poate
mai
puncte de vedere. Implantul trebuie să posede calită i
mult sau mai pu in tolerant fa ă de el. Dacă toleran a
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
99
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
este bună, organismul îl îmbracă de jur împrejur cu
esut propriu. Sub această formă el poate să rămână în
organism perioade lungi de timp, deoarece organismul
chiar dacă nu-l va considera niciodată ca pe o
componentă proprie, nu va declanşa în mod normal
reac ii de respingere nici ulterior perioadei de integrare a
lui.
Construc ia implantului se referă la forma,
dimensiunile, prezen a sau nu a unor structuri de
ancorare în esut (dacă prezintă let, pasul şi înăl imea
acestuia), dar şi la proprietă ile sale mecanice (duritatea
şi rezisten a).
Biomecanica se referă la proprietă ile mecanico-
dinamice ale unui implant în rela ie cu esuturile
înconjurătoare, la cât de bine este el ancorat în structurile
Figura 1. Sala de opera ie prezintă condi iile
și principiile unei interven ii operatorii în
organismului.
condi ii sterile
Pentru testarea biocompatibilită ii şi rezisten ei
implanturilor se procedează la inserarea lor în os cortical
sau trabecular la animale de experien ă, în condilul
femural, dia za oaselor lungi, maxilar sau mandibulă
[2]. Pentru evaluarea rezultatelor ob inute pe parcursul
perioadei experimentale se poate apela la microscopie
optică sau electronică, ecare cu avantaje şi limite [3].
Microscopia optică are marele avantaj că permite
ob inerea de informa ii amănun ite despre întreaga zonă
de esut care con ine implantul, de la interfa a os-
implant până în profunzimea esuturilor proliferate în
jurul implantului. Prelucrarea histopatologică a
esuturilor proliferate în jurul implantului este însă
foarte laborioasă, astfel că este di cilă procesarea seriilor
mari de probe. Laboratoarele dotate cu microtoame
speciale care pot sec iona oase nedecalci cate oferă
Figura 2. Implantele de zirconiu și titan la
posibilită i de ob inere de informa ii într-o perioadă
nivelul femurului prezintă stabilitate primară
mai scurtă de timp comparativ cu prelucrarea clasică
prin decalci care şi includere în para nă [4,5]. Având în
vedere bogă ia de informa ii pe care le poate furniza,
În acest studiu s-au utilizat 8 iepuri de casă, rasă
microscopia optică este considerată încă cea mai bună
comună (metişi) în vârstă de
7 luni, proveni i din
metodă pentru a evalua răspunsul esutului la un
biobaza Universită ii de Medicină şi Farmacie Oradea; 4
material de implant [3].
iepuri de sex masculin cu greutate între 3,5-4 kg și
Scopul acestei lucrări este acela de a testa in uen a
lungimea între 40- 45 cm și 4 iepuri de sex feminin cu
implanturilor de titan și zirconiu asupra osteointegrării
greutatea cuprinsă între 4-5 kg și lungimea de 40-50
și osteogenezei, de a urmări modi cările histopatologice
cm. Iepurii au fost împăr i i în 2 loturi. La primul lot au
perimplant pentru a ști care este cel mai potrivit
fost inserate implanturi de titan (1AT), la al doilea de
biomaterial, cu proprietă ile cele mai avantajoase.
titan și zirconiu. Implantarea femurului cu implante de
titan și/sau zirconiu și ulterior sacri carea iepurilor s-a
Material și metodă
efectuat într-o sală de opera ie, respectându-se întrutotul
condi iile și principiile unei interven ii operatorii.
Materialele testate în acest experiment pe iepuri
Această sală de opera ie apar ine unei clinici veterinare
sunt implanturi de titan și zirconiu (formă tronconică,
(Figura 1).
cu let, lungime
5 mm) comandate și produse
Implanturile au fost selectate și sterilizate. Ele au
personalizat de S.C. Tehnomed Impex Co. SA București,
fost implantate în condi ii chirurgicale în femur de
o companie specializată în materiale sanitare.
iepure, la 1 cm de distan ă între cele două implanturi.
100
Bumbu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figura 3. Aspectul macroscopic al femurului
Figura 5. Lot 1AT - osul în care a fost inserat
prelevat pentru studiu
implantul de titan, aspect la 3 săptămâni
postoperator. Grosimea osului dia zar creşte
uşor şi progresiv pe măsura apropierii
de implant (Tricrom Goldner)
Figura 4. Sec ionarea femurului în vederea
prelucrării histologice
Dimensiunea implantelor a fost de aproximativ 1,5 cm,
Figura 2.
Figura 6. Lot 1AT - osul în care a fost inserat
Experimentul a durat 4 luni. În acest articol ne vom
implantul de titan, aspect la 3 săptămâni
referi la modi cările periimplant aparute în primele 3
postoperator. Rezorb ia osului necrozat şi
săptămâni după implantare.
înlocuirea par ială cu os nou format
Pe tot parcursul experimentului, iepurii au bene ciat
(Tricrom Goldner)
de condi ii corespunzătoare şi controlate în permanen ă:
temperatura 20-24oC şi lumină naturală, cu un ciclu
lumină-întuneric aproximativ 12/12 ore. Animalele au
conjunctiv care a acoperit implantul până în cavitatea
fost hrănite pe întreaga perioadă experimentală cu furaj
medulară (Figura 5). Dacă urmărim grosimea osului
granulat standardizat şi au bene ciat de apă proaspătă la
dia zar constatăm că acesta creşte uşor şi progresiv pe
discre ie.
măsură ce ne apropiem de zona implantului şi creşte
La sfârşitul perioadei experimentale animalele au
semni cativ în imediata apropiere a acestuia.
fost sacri cate şi s-a recoltat femurul
(Figura
3) în
Îngroşarea peretelui dia zar din vecinătatea
vederea efectuării de examene histopatologice. Cu freza
implantului are loc atât spre profunzime (proemină spre
stomatologică au fost sec ionate capetele osoase la
cavitatea medulară), cât şi spre suprafa ă. Aspectul şi
aproximativ 1 cm de la implant (Figura 4) şi piesele
structura osului din vecinătatea implantului nu sunt
astfel fasonate au fost introduse imediat în formol 10%
identice pe toată suprafa a, existând diferen e mari de la
pentru xare. După decalci care, piesele au fost incluse
o zonă la alta. Astfel, zona mijlocie con ine os modi cat
în para nă. S-au practicat sec iuni seriate cu grosime de
structural în urma traumatismului din timpul efectuării
5 µ, care au fost colorate cu metoda tricromă Goldner.
defectului experimental necesar inserării implantului.
Acest traumatism a fost urmat de necroză osoasă zonală
Rezultate
ce a pătruns până la o anumită adâncime în peretele osos.
Chiar dacă se observă o anumită activitate
Sec iunile histologice seriate efectuate prin osul în
reparatorie ce înaintează din profunzimea osului spre
care a fost inserat implantul de titan au permis aprecieri
suprafa a de contact cu implantul, rezorb ia osului
asupra întregii zone de implantare, de la esutul
necrozat şi înlocuirea lui cu os nou format s-au realizat
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
101
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
doar par ial până la acest moment al experimentului, cu
Aspectele care interesează cel mai mult sunt cele
diferen e de la o zonă la alta. (Figura 6).
existente la interfa a os-implant şi ele pot
apreciate
Cu totul alta este situa ia în zonele super cială şi
foarte bine pe sec iunea histologică. Se poate observa că
profundă a osului dia zar din vecinătatea implantului,
peretele osos urmăreşte intim suprafa a implantului de
unde osul este în plin proces de proliferare şi extindere,
la suprafa ă şi până în canalul medular.
astfel încât suprafa a de contact cu implantul este
Per total suprafa ă, osteointegrarea pare în stadiu
evident mai mare decât grosimea ini ială a osului
ceva mai avansat decât în cazul implantului de titan,
dia zar. Osul de la suprafa a defectului experimental
zona de os afectat ce urmează a eliminat treptat este
apare necrozat doar pe o zonă sub ire (cea care vine în
aici evident mai sub ire (Figura 10).
contact intim cu implantul) şi în rest are aspect de os
Şi în cazul implantului de zirconiu peretele dia zar
trabecular cu tendin ă evidentă de proliferare şi
din imediata vecinătate a implantului s-a îngroşat, dar
extindere. Astfel, pornind dinspre implant, osul de la
nu în ambele sensuri ca în cazul implantului de titan.
suprafa a dia zei prezintă din loc în loc areole şi tendin ă
Peretele dia zar nu numai că nu s-a îngroşat spre
de proliferare spre periost e prin formarea de noi
exterior, dar treimea externă din contact cu implantul
trabecule, e prin proliferarea de os subperiostal cu
prezintă os afectat pe cea mai profundă zonă din tot
aspect de os primar în care se observă o oarecare tendin ă
peretele dia zar şi nici nu se constată procese de
de formare a unor areole. Areolele existente în toate
proliferare de os periostal la nivelul celui existent în
aceste zone con in osteoblaste în număr mare (Figura
cazul imlantului de titan. O tendin ă discretă de
7), ceea ce sugerează că proliferarea osoasă este intensă.
proliferare a osului în zona subperiostală se constată
Acest os tânăr ce se organizează treptat în zona
doar la o anumită distan ă de zona implantului.
subperiostală va constitui o structură de rezisten ă
Cu totul alta este situa ia în treimea centrală şi mai
necesară consolidării zonei implantului care a fost slăbită
ales cea internă a zonei implantului unde refacerea
mecanic după efectuarea defectului osos experimental.
esutului osos poate considerată foarte bună, având în
Concomitent cu procesele de proliferare osoasă se
vedere că au trecut doar trei săptămâni de la interven ie.
derulează şi procese de rezorb ie osoasă necesară
Aici există doar o fâşie foarte sub ire de os afectat, în
îndepărtării tuturor structurilor osoase afectate în urma
contact intim cu implantul, dar după aspect acesta va
traumatismului operator. Existen a rezorb iei osoase este
resorbit în timp relativ scurt şi înlocuit cu os nou format.
ilustrată de existen a osteoclastelor a ate în contact
Osul dia zar din zona implantului se continuă spre
intim cu osul afectat (Figura 8).
interiorul cavită ii dia zare cu o prelungire osoasă care
Zona profundă a peretelui osos din vecinătatea
urmăreşte intim implantul, iar ca structură este os relativ
implantului este format din os trabecular ce depăşeşte
areolar cu aspect tipic de os tânăr [6]. Areolele acestui os
semni cativ marginea internă a osului dia zar. Este
con in numeroase osteoblaste ceea ce demonstrează că el
vorba de os areolar nou format, în care se mai pot observa
se a ă în plin proces de proliferare (Figura 11).
rare fragmente osoase cu aspect vestigial rămase în urma
La partea internă a osului dia zar se constată şi în
traumatismului determinat de executarea defectului osos
cazul acestui implant, îngroşarea peretelui osos prin
experimental. Trabeculele acestui os areolar con in la
proliferarea unui manşon osos, ce poate urmărit pe o
periferia lor un număr impresionant de osteoblaste, ceea
distan ă relativ mare şi care se sub iază pe măsura
ce demonstrează că activitatea de proliferare osoasă este
îndepărtării de zona implantului. El reprezintă şi aici o
aici în plină desfăşurare. Acest os trabecular se continuă
structură de consolidare internă pentru a compensa
la partea dia zei dinspre canalul medular cu o por iune
slăbirea rezisten ei mecanice de moment a zonei
de os par ial areolar, a cărei grosime descreşte pe măsura
implantului.
îndepărtării de zona implantului. Este vorba tot de o
Concomitent cu aceste procese active de proliferare
structură de rezisten ă care consolidează la interior osul
osoasă au fost identi cate şi aspecte legate de liza
care înconjoară implantul. Atât în areolele acestui
structurilor osoase necesară eliminării componentelor
manşon osos, cât şi la suprafa a lui, există numeroase
osoase compromise în momentul efectuării defectului
osteoblaste, ceea ce sugerează că aceste structuri de
experimental şi afectate de procesele in amatorii şi
consolidare se vor extinde în continuare.
necrotice postoperatorii. Existen a lor este ilustrată de
Imaginea de ansamblu oferă informa ii despre zona
prezen a osteoclastelor atât în zona de contact cu
implantului de zirconiu şi efectul acestuia asupra
implantul, cât şi la o oarecare distan ă de acesta. În
structurilor dure şi moi pe o distan ă care permite
zonele în care au rămas fragmente osoase despinse în
aprecierea efectelor traumatismului operator şi a proceselor
momentul efectuării defectului osos experimental,
de refacere până la o distan ă mare de implant (Figura 9).
numărul osteoclastelor este foarte mare (Figura 12).
102
Bumbu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figura 7. Lot 1AT - osul în care a fost inserat
Figura 10. Lot 1AZ - osul în care a fost
implantul de titan, aspect la 3 săptămâni
inserat implantul de zirconiu, aspect la 3
postoperator. Densitatea osteoblastelor
săptămâni postoperator. Evolu ia comparativă
în procesul de proliferare osoasă
a osteointegrării pentru cele două tipuri
(Tricrom Goldner)
de implant (Tricrom Goldner)
Figura 8. Lot 1AT - osul în care a fost inserat
Figura 11. Lot 1AZ - osul în care a fost
implantul de titan, aspect la 3 săptămâni
inserat implantul de zirconiu, aspect la 3
postoperator. Prezen a osteoclastelor a ate
săptămâni postoperator. Procesul de proliferare
în contact intim cu osul afectat
osoasă eviden iat prin prezen a numărului
(Tricrom Goldner)
mare de osteoblaste (Tricrom Goldner)
Figura 9. Lot 1AZ - osul în care a fost inserat
Figura 12. Lot 1AZ - osul în care a fost
implantul de zirconiu, aspect la 3 săptămâni
inserat implantul de zirconiu, aspect la 3
postoperator. Efectele traumatismului operator şi
săptămâni postoperator. Prezen a osteoclastelor
a proceselor de refacere în raport cu distan a fa ă
la nivelul defectului osos experimental
de implant (Tricrom Goldner)
(Tricrom Goldner)
Discuții
intim cu materialul implantului, urmărind toate
denivelările acestuia. Nu se constată reac ie de respingere
Urmărind esuturile osoase din jurul celor două
de către organism în cazul niciunuia dintre implanturile
tipuri de implanturi constatăm că ele se a ă în contact testate. Leziunile consecutive efectuării defectului
Histopathological Comparative Assessment of Osseointegration Processes of Titanium and Zirconium Dental Implants in
103
the Rabbit Femur
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
experimental în care s-a inserat implantul au dispărut în
proces de derulare şi la o intensitate foarte bună, osul
cea mai mare parte prin proliferare de structuri osoase
nou format îmbrăcând deja implanturile pe o anumită
tinere care au înaintat din profunzimea osului spre
suprafa ă şi prezintă tendin ă clară de extindere în
suprafa a de contact cu implantul. Pe cea mai mare parte
continuare. Procesele de osteointegrare se derulează la
din suprafa a de contact cu implantul, osul este refăcut
nivel comparabil în cazul celor două tipuri de implanturi,
deşi el are încă aspect de os tânăr, care va mai suferi
dar există totuşi o mică diferen ă în favoarea celui de
procese treptate de remaniere şi consolidare. Procesele
zirconiu, unde proliferarea osoasă pare ceva mai
reparatorii au evoluat atât de bine încât osul nou format
avansată.
se extinde peste denivelările implantului pe o anumită
distan ă, ceea ce face ca suprafa a os-implant să e mai
groasă decât cea a osului dia zar în care s-a practicat
Referințe
defectul osos. Această extindere a osului nou format are
loc în primul rând la partea internă a defectului
1.
Osborn JF, Newesley H. Dynamics aspects of the bone-
experimental şi lasă impresia că va continua îmbrăcând
implant interface. In Heimke G, ed: Dental implants-
implantul cu structuri osoase pe suprafa ă din ce in ce
material and systems. Hanser, Munich, 1980;pp 111-
mai mare. Mai mult, osul nou format se extinde la partea
23.
internă a osului dia zar pe o anumită distan ă, ceea ce
2.
Tencer AF. Osteocompatibility. In von Recum AF, ed:
duce la îngroşarea zonală şi creşterea rezisten ei osului
Handbook of Biomaterials Evaluation. Taylor and
dia zar din jurul implantelor. Aceste aspecte arată o
Francis, Philadelphia, PA, 1999:539-66.
evolu ie foarte favorabilă a proceselor de osteointegrare,
3.
John A. Jansen. Histological Analysis of Bone-Implant
chiar dacă până la nalizarea acestora mai trebuie să
Interface. From: Handbook of Histology Methods for
treacă o perioadă lungă de timp. Cele numai 3 săptămâni
Bone and Cartilage, Edited by: Y. H. An and K. L.
care au trecut de la inserarea implaturilor sunt insu ciente
Martin, Humana Press Inc., Totowa, NJ, 2003, 353-
pentru nalizarea proceselor de osteointegrare. Aspectul
60.
este ilustrat de faptul că la interfa a os-implant mai poate
4.
Donath K, Breuner G. A method for the study of
eviden iat os acelular degenerat, dar numai pe zone
undecalci ed bones and teethwith attached soft tissues.
circumscrise, a ate şi acestea doar în jumătatea externă a
e Säge-Schli
(sawing and grinding) technique. J
osului dia zar. Grosimea acestui os degenerat este pu in
Oral Pathol 1982;11(4):318-26.
diferită de la o zonă la alta, dar per total interfa ă os-
5.
van der Lubbe HB, Klein CP, de Groot K. A simple
implant diferen ele nu sunt semni cative între cele două
method for preparing thin
(10microM) histological
tipuri de implanturi. Se pare totuşi că la acest moment al
sections of undecalci ed plastic embedded bone with
experimentului, procesele de osteointegrare sunt sensibil
implants. Stain Technol 1988;63(3):171-6.
mai avansate în cazul implantului de zirconiu.
6.
Erlandsen S L, Magney J E. Color Atlas of Histology,
Mosby Year Book, St. Louis, 1992
Concluzii
7.
Black J. Biological Performance of Materials. Marcel
Dekker Inc., New York, NY, 1992.
La trei săptămâni de la inserarea celor două tipuri de
8.
Carl Hanser Verlag. Dental Implants: Materials and
implanturi procesele de osteointegrare se a ă în plin
Systems. Munich, Germany, 1980:111-23.
104
Bumbu et al
ORIGINAL ARTICLES
URMĂRIREA CAZURILOR DE ABDOMEN ACUT LA PACIENȚII
DIABETICI COMPARATIV CU CEI NONDIABETICI
Dănu Dejeu1,2, Aurel Babeș2
1Clinica de Chirurgie I, Spitalul Clinic Jude ean de Urgen ă Oradea, 2Facultatea de Medicină și Farmacie din cadrul
Universită ii din Oradea
Adresa pentru coresponden ă:
Dr. Dănu Dejeu
Str. Gh. Doja nr. 184 A, Oradea
E-mail: dandejeu@yahoo.com
Primit: 01.09.2014
Acceptat: 30.09.2014
Med Con October 2014, Vol 9, No 3, 105-114
Motto: „Mai bine să regretăm la masa de opera ie decât la cea de autopsie” - I. IACOBOVICI
Rezumat
diabetici este semni cativ mai mare decât la nondiabetici
(9,84% vs. 5,38%). Durata medie de spitalizare în
Introducere: Ne-am propus să analizăm impactul
Clinica de Chirurgie I este de
3,8 zile. În cazul
hiperglicemiei asupra evolu iei pacien ilor cu diabet
abdomenului acut, spitalizarea pacien ilor nondiabetici
zaharat și abdomen acut comparativ cu pacien ii
este de 5,1 zile, iar în cazul pacien ilor diabetici durata
nondiabetici, privind rata morbidită ii și mortalită ii,
medie de spitalizare este de 7,8 zile.
durata spitalizării.
Concluzii: Studiul demonstrează diferen ele în ceea
Metode: Acest studiu observa ional, retrospectiv și
ce privește evolu ia pacien ilor, complica iile survenite,
de cohortă s-a desfășurat în perioada 2008-2011, pe un
mortalitatea precum și durata de spitalizare.
număr de 4021 cazuri cu abdomen acut internate în
Cuvinte cheie: abdomen acut, diabetici,
Clinica de Chirurgie I a Spitalului Clinic Jude ean de
nondiabetici, morbiditate, mortalitate
Urgen ă Oradea. Dintre acestea, 488 au fost pacien i
diabetici şi 3533 pacien i nondiabetici.
Introducere
Rezultate: La ambele loturi au predominat femeile
(62,24% vs. 58,40%). Majoritatea pacien ilor (62,37%)
Abdomenul acut poate
de nit ca un proces
cu abdomen acut au avut vârste cuprinse între 30-69
patologic intraabdominal cauzând în general, durere
ani, cu diferen ă semni cativă statistic
(p<0,0001).
puternică și care necesită o decizie imediată, în majoritatea
Forma vasculară, pancreatita acută şi falsul abdomen
cazurilor, interven ie chirurgicală [1,2]. Cauzele generale
acut au fost semni cativ mai frecvente la pacien ii
care ar putea-o produce sunt împăr ite în 5 categorii:
diabetici fa ă de cei nondiabetici. Forma peritonitică a
in amatorii, mecanice, vasculare, traumatice, pancreatita
fost mai frecventă la nondiabetici, cu diferen ă
acută [3]. Cauzele in amatorii se pot împăr i în două
semni cativă statistic (p=0,0003). La pacien ii diabetici
categorii: bacteriană (apandicita acută, diverticulita acută,
morbiditatea postoperatorie a fost la
36,27% dintre
colecistita acută) și chimică
(ulcer gastro-duodenal
pacien ii opera i, procent semni cativ mai mare decât la
perforat). Cauzele mecanice se referă la herniile încarcerate,
pacien ii nondiabetici
(14,43%). Mortalitatea la
aderen e postoperatorii, torsiune, obstruc ii neoplazice
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
105
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabel I. Distribu ia cazurilor cu abdomen acut internate în Clinica de Chirurgie I
a Spitalului Clinic Jude ean de Urgen ă Oradea, în func ie de sex
Anul 2008
Anul 2009
Anul 2010
Anul 2011
Total
Sex
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nondiabetici
Femei
460
61,17
493
63,53
502
62,67
744
61,79
2199
62,24
Bărba i
292
38,83
283
36,47
299
37,33
460
38,21
1334
37,76
752
776
801
1204
3533
p†
p<0,0001*
Diabetici
Femei
67
58,26
64
57,66
60
57,69
94
59,49
285
58,40
Bărba i
48
41,74
47
42,34
44
42,31
64
40,51
203
41,60
115
111
104
158
488
p†
p=0,0004*
Total
Femei
527
60,78
557
62,80
562
62,10
838
61,53
2484
61,78
Bărba i
340
39,22
330
37,20
343
37,90
524
38,47
1537
38,22
867
887
905
1362
4021
p†
p<0,0001*
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
ale colonului. Categoria vasculară - produc abdomen
Studiul a fost aprobat de comisia de avizare internă
acut prin tromboză sau embolie mezenterică urmată de
a lucrărilor de cercetare-dezvoltare din cadrul spitalului.
necroza și gangrena intestinală. Cauzele traumatice se
Ca metode de analiză statistică au fost folosite testul
referă la plăgile abdominale deschise, traumatisme
Chi-pătrat, Fisher’s exact test, Comparison of means
abdominale cu ruptură de splină sau cat [4].
test, Comparison of proportions test, Relative risk test şi
Este esen ial să recunoaștem o urgen ă abdominală
calcularea coe cientului de corela ie utilizând programul
acută pentru care o interven ie chirurgicală este necesară
de statistică medicală MedCalc® versiunea
12.2.1.0
și nu trebuie să e amânată [5]. Pacien ii se prezintă cu
(MedCalc® Software, Mariakerke, Belgium).
diverse combina ii de simptome cum ar durere, colaps,
șoc, dar nu toate aceste caracteristici clinice sunt prezente
Rezultate
la ecare pacient [6]. Durerea severă este simptomul cel
mai frapant și este adesea generalizată
[7]. Dilema
Pacien i
esen ială se ridică în fa a unui bolnav diabetic cu
În perioada studiată au predominat femeile (61,78%
cetoacidoză și semne de abdomen acut. Instalarea
vs. 38,22%), rezultând un raport femei/bărba i de 1,6:1.
cetoacidozei poate
consecin a unei afec iuni
La nondiabetici raportul femei/bărba i a fost de 1,6, iar
nechirurgicale, iar semnele digestive se datorează
la diabetici raportul a fost de 1,4 (Tabel I).
decompensării metabolice, sau poate secundară unui
Analizând distribu ia cazurilor în func ie de vârstă,
veritabil abdomen acut [8]. Ne-am propus să determinăm
putem observa că majoritatea pacien ilor (62,37%) cu
impactul hiperglicemiei peri-, intra- și post-operatorii
abdomen acut au avut vârste cuprinse între 30-69 ani, cu
asupra evolu iei pacien ilor cu diabet zaharat și abdomen
diferen ă semni cativă statistic (p<0,0001) (Tabel II).
acut, comparativ cu pacien ii nondiabetici, privind rata
Vârsta medie la diabetici a fost semni cativ mai
morbidită ii și mortalită ii, durata spitalizării.
mare decât la nondiabetici (62,14 ani vs. 49,37 ani)
(p<0,0001) (Tabelul nr. II).
Material și metode
În lotul pacien ilor nondiabetici cu abdomen acut
peste 60% au avut vârste cuprinse între 30-69 ani, cu
Acest studiu observa ional, retrospectiv și de cohortă
diferen ă semni cativă statistic (p<0,0001), în timp ce în
s-a desfășurat în perioada 2008-2011, pe un număr de
lotul pacien ilor diabetici cu abdomen acut majoritatea
4021 cazuri cu abdomen acut, internate în Clinica de
(85,86%) au avut vârste peste 50 ani, (p<0,0001) (Tabel II).
Chirurgie I a Spitalului Clinic Jude ean de Urgen ă
Diabetul zaharat tip I a fost prezent doar la 4,10%
Oradea. Dintre acestea, 488 au fost pacien i diabetici şi
dintre pacien ii diabetici, majoritatea având diabet
3533 pacien i nondiabetici.
zaharat tip II (95,90%) (p<0,0001) (Tabel III).
106
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Tabel II. Distribu ia cazurilor cu abdomen acut internate în Clinica de Chirurgie I
a Spitalului Clinic Jude ean de Urgen ă Oradea, în func ie de vârstă
Anul 2008
Anul 2009
Anul 2010
Anul 2011
Total
Vârsta
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nr.
%
Nondiabetici
<30
168
22,34
161
20,75
180
22,47
249
20,68
758
21,45
30-49
196
26,06
209
26,93
219
27,34
295
24,50
919
26,01
50-69
262
34,84
272
35,05
273
34,08
439
36,46
1,246
35,27
≥70
126
16,76
134
17,27
129
16,10
221
18,36
610
17,27
p†
p<0,0001*
V. medie
48,83±5,52
49,06±6,01
48,46±5,78
50,25±5,87
49,37±5,72
Diabetici
<30 years
3
2,61
2
1,80
2
1,92
6
3,80
13
2,66
30-49
11
9,57
13
11,71
15
14,42
17
10,76
56
11,48
50-69
68
59,13
68
61,26
60
57,69
91
57,59
287
58,81
≥70
33
28,70
28
25,23
27
25,96
44
27,85
132
27,05
p†
p<0,0001*
V. medie
62,81±7,21
62,34±6,97
61,59±7,14
61,87±7,26
62,14±6,92
p†
Non-diabetic
49,37±5,72
Diabetic
62,14±6,92
p<0,0001**
Total
<30
171
19,72
163
18,38
182
20,11
255
18,72
771
19,17
30-49
207
23,88
222
25,03
234
25,86
312
22,91
975
24,25
50-69
330
38,06
340
38,33
333
36,80
530
38,91
1,533
38,12
≥70
159
18,34
162
18,26
156
17,24
265
19,46
742
18,45
p†
p<0,0001*
V. medie
50,69±6,45
51,06±6,24
49,97±6,05
51,60±5,75
50,92±6,15
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Chi-square test
** Comparison of means test
Majoritatea cazurilor au avut o durată de evolu ie a
diabetului de peste
10 ani
(34,43%). Remarcăm
Tabel III. Caracteristici ale pacien ilor diabetici
procentul important al pacien ilor diagnostica i cu
cu abdomen acut
diabet zaharat la internare (16,39%) (Tabel III).
Majoritatea diabeticilor au avut terapie cu
Tip diabet zaharat
Nr.
%
p†
antidiabetice orale
(57,79%). Insulinodependen ii au
DZ tip 1
20
4,10
reprezenat 25,82%, din care 15,16% au urmat terapie
p<0,0001*
DZ tip 2
468
95,90
mixtă
(ADO+insulină). Procentul celor fără terapie
Durata diabet zaharat
(16,39%) reprezintă cazurile depistate cu diabet la
Diagnostic la internare
80
16,39
internare (Tabel III).
<1 an
61
12,50
Analizând durata medie de la debut la internare a
1-5 ani
100
20,49
p<0,0001*
abdomenului acut, s-a constatat că aceasta a fost în medie
5-10 ani
79
16,19
cu 33,52 ore înainte de internare, durată semni cativ
mai mare la bărba i fa ă de femei (35,64 ore vs. 32,21
>10 ani
168
34,43
ore) (p<0,0001) (Tabelul nr. IV). La nondiabetici durata
Terapia antidiabetică
de la debutul bolii la internare a fost semni cativ mai
Fără terapie
80
16,39
mare la bărba i decât la femei (34,56 ore vs. 29,04 ore)
ADO
282
57,79
p<0,0001*
(p<0,0001), în timp ce la diabetici această durată a fost
Insulină
52
10,66
semni cativ mai mare la femei decât la bărba i (56,64
ADO + insulina
74
15,16
ore vs. 42,72 ore) (p<0,0001). Durata de la debutul
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile
afec iunii abdominale la internare a fost semni cativ mai
studiate
mare la pacie ii diabetici fa ă de cei nondiabetici (50,85
* Chi-square test
ore vs. 31,20 ore) (p<0,001) (Tabel IV).
ADO - antidiabetice orale
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
107
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabel IV. Durata de timp de la debut la internare (ore) a pacien ilor suferind de abdomen acut
Pacien i
Femei
Bărba i
p†
Total
p†
Nondibaetici
29,04±3,75
34,56±4,50
p<0,0001*
31,20±4,27
p<0,0001*
Diabetici
56,64±6,86
42,72±5,32
p<0,0001*
50,85±6,28
Total
32,21±4,87
35,64±4,72
p<0,0001*
33,52±4,92
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Comparison of means test
Tabel V. Nivelul mediu al glicemiei la pacien ii lua i în studiu, suferind de abdomen acut
Total pacien i
Nondiabetici
Diabetici
Valoarea medie a glicemiei (mg/dl)
p†
(n=4021)
(n=3533)
(n=488)
Înainte de interven ia chirurgicală
120,4±37,9
112,6±28,2
154,42±17,82
p<0,0001*
În ziua interven iei chirurgicale
137,6±33
132,2±27,6
160,89±19,44
p<0,0001*
După interven ia chirurgicală medie
119,9±26,5
114,5±21,2
147,91±19,20
p<0,0001*
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
*Comparison of means test
Tabel VI. Distribu ia cazurilor în func ie de forma clinică abdomenului acut
Nondiabetici
Diabetici
Total
Forma
p†
Nr.
% Nr.
% Nr.
%
Peritonitic
2158
61,08
256
52,46
2414
60,03
p=0,0003*
Ocluziv
894
25,30
121
24,80
1015
25,24
p=0,8516*
Hemoragic
142
4,02
22
4,51
164
4,08
p=0,6967*
Torsiune de organ
28
0,79
7
1,43
35
0,87
p=0,2416*
Vascular
34
0,96
20
4,10
54
1,34
p<0,0001*
Pancreatita acută
256
7,25
52
10,66
308
7,66
p=0,0103*
Fals abdomen acut
21
0,59
10
2,05
31
0,77
p=0,0015*
Total
3533
488
4021
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Chi-square test
Nivelul glucozei din sânge înainte de interven ia
Forme clinice
chirurgicală în întreaga cohortă a fost de 120,4±37,9 mg/dl.
Cea mai frecventă formă de abdomen acut a fost cea
Cum era de așteptat, subiec ii nondiabetici au avut niveluri
peritonitică (60,03%), urmată de cea ocluzivă (25,24%).
mai mici ale glicemiei pre-operator (112,6±28,2 mg/dl)
Pancreatita acută a reprezentat 7,66% dintre cazuri, iar
comparativ cu pacien ii cu antecedente cunoscute de diabet
forma hemoragică s-a întâlnit la 4,08%. Restul formelor
(154,42±17,83 mg/dl, p<0,0001). Nivelul de glucoză din
au avut procente mai mici de 1,5% (Tabel VI).
sânge în prima zi după opera ie a fost de 160,89±19,44 mg/
Forma vasculară, pancreatita acută şi falsul abdomen
dl la pacien ii cu diabet zaharat și 132,2±27,6 mg/dl la
acut au fost semni cativ mai frecvente la pacien ii
subiec ii nondiabetici; ambele valori au fost mai mari decât
diabetici fa ă de cei nondiabetici (4,10% vs. 0,96%,
cele raportate în timpul spitalizării ulterior (147,91±19,20
p<0,0001;
10,66% vs.
7,25%, p=0,0103, respectiv
și 114,5±21,2 mg/dl, respectiv, p<0,0001) (Tabel V).
2,05% vs. 0,59%, p=0,0015) (Tabel VI).
După opera ie,
39,99%
(192) dintre pacien ii
Forma peritonitică a fost mai frecventă la
diabetici au avut o glicemie >140 mg/dl; trei sferturi
nondiabetici, cu diferen ă semni cativă statistic
dintre aceștia (144) au avut glicemia între 141 și 180
(p=0,0003), iar formele ocuzivă, hemoragică şi torsiunea
mg/dl, iar restul (48) au avut glicemia >180 mg/dl.
de organ au fost mai frecvente la diabetici, dar fără a
Clinic, hiperglicemia semni cativă
(de nită ca
exista diferen e semni cative (p>0,05) (Tabel VI).
glucoză în sânge >180 mg/dl) a fost observată la 7,78%
Abdomenul acut peritonitic
(38) dintre pacien ii diabetici înainte de interven ia
Cele mai frecvente cauze ale abdomenului acut
chirurgicală, la 17,2% (84) dintre pacien ii diabetici în
peritonitic în întregul lot (diabetici+nondiabetici) au fost
ziua opera iei și la 9,83% (48) dintre pacien ii diabetici
apendicita acută (24,73%), colecistita acută (22,12%),
în perioada postoperatorie (2-10 zile).
perfora ii ale intestinului sub ire şi gros
(17,94%) şi
108
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Tabel VII. Distribu ia pacien ilor cu abdomen acut peritonitic în func ie de leziunea determinantă
Nondiabetici
Diabetici
Total
Cauze
p†
Nr.
%
Nr.
%
Nr.
%
Apendicita acută
544
25,21
53
20,70
p=0,5761*
597
24,73
Colestistita acută
486
22,52
48
18,75
p=0,6762*
534
22,12
Diverticulita acută
178
8,25
28
10,94
p=0,9130*
206
8,53
Ulcer gastro-duodenal perforat
286
13,25
26
10,16
p=0,8855*
312
12,92
Perfora ii intestin sub ire și gros
391
18,12
42
16,41
p=0,9499*
433
17,94
Peritonita biliară
40
1,85
12
4,69
p=0,6164*
52
2,15
Afec iuni ginecologice - pelviperitonită
41
1,90
8
3,13
p=0,2603*
49
2,03
Dializa peritoneală
6
0,28
2
0,78
p<0,0001*
8
0,33
Abces hepatic/splenic rupt
7
0,32
3
1,17
p<0,0001*
10
0,41
Postoperatorii
153
7,09
25
9,77
p=0,9503*
178
7,37
Colec ii perinefritice rupte în peritoneu
2
0,09
2
0,78
p<0,0001*
4
0,17
Peritonita primitivă
5
0,23
2
0,78
p<0,0001*
7
0,29
Altele
19
0,88
5
1,95
p=0,0276*
24
0,99
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
Tabel VIII Germenii implica i în abdomenul acut peritonitic
Nondiabetici
Diabetici
Total
Cauze
p†
Nr.
%
Nr.
%
Nr.
%
E. coli
1.467
67.98
143
55.86
p=0.0044*
1.610
66.69
Pseudomonas
486
22.52
48
18.75
p=0.6762*
534
22.12
Proteus
178
8.25
28
10.94
p=0.9130*
206
8.53
Seratia
286
13.25
26
10.16
p=0.8855*
312
12.92
Candida
391
18.12
42
16.41
p=0.9499*
433
17.94
Aerobacter
40
1.85
12
4.69
p=0.6164*
52
2.15
Klebsiella
41
1.90
8
3.13
p=0.2603*
49
2.03
Anaerobi
6
0.28
2
0.78
p<0.0001*
8
0.33
Bacteridis
7
0.32
3
1.17
p<0.0001*
10
0.41
Streptococi
153
7.09
25
9.77
p=0.9503*
178
7.37
Sta lococi anaerobi
2
0.09
2
0.78
p<0.0001*
4
0.17
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
ulcere gastro-duodenale perforate (12,92%), urmate de
Durata medie de spitalizare la abdomenul acut
diverticulita acută (8,53%) şi complica ii postoperatorii
peritonitic a fost de 5,29 zile, semni cativ mai mare la
(7,37%), cu procente semni cativ mai mici, restul
diabetici fa ă de nondiabetici
(6,80 vs.
5,11 zile)
cauzelor având procente sub 3% (Tabel VII).
(p<0,0001).
Din punct de vedere al leziunilor determinante
Abdomenul acut ocluziv
există diferen e semni caive între diabetici şi
Atât la diabetici, cât şi la nondiabetici, cele mai
nondiabetici în cazul dializei peritoneale, abcesului
frecvente leziuni primare în abdomenul acut ocluziv au
hepatic/splenic şi a colec iilor perinefritice rupte,
fost eventra iile şi herniile (40,50% vs. 39,37%), urmate
peritonitei primitive și altor cauze (p<0,05).
de cauzele parietale (tumori, in ama ii, stenoze) (29,75
Analizând frecven a germenilor implica i în
vs. 31,54%) şi cele extraparietale (23,14% vs. 20,13%),
abdomenul acut peritonitic, am constatat că E. coli a
neexistând diferen e semni cative între cele două loturi
fost germenul implicat la majoritatea cazurilor
(p>0,05). Durata medie de spitalizare la abdomenul
(66,69%), atât la diabetici, cât şi la nondiabetici cu
acut ocluziv a fost de 5,29 zile, semni cativ mai mare la
diferen ă semni cativă statistic între cele două loturi în
diabetici fa ă de nondiabetici
(6,80 vs.
5,11 zile)
compara ie cu al i germeni (p=0,0044) (Tabel VIII).
(p<0,0001) (Tabel IX).
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
109
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabel IX. Distribu ia pacien ilor cu abdomen acut ocuziv în func ie de leziunea primară
și durata medie de spitalizare (DMS)
Nondiabetici
Diabetici
Total
p†
Nr.
%
Nr.
%
Nr.
%
Extraparietale (tumori abdominale
180
20,13
28
23,14
p=0,9082*
208
20,49
comprensive, bride, aderen e)
Parietale (tumori, in ama ii, stenoze)
282
31,54
36
29,75
p=0,9783*
318
31,33
Intraluminale (fecalom, calculi biliari,
32
3,58
4
3,31
p=0,1599*
36
3,55
corpi străini)
Eventra ii, hernii
352
39,37
49
40,50
p=0,9965*
401
39,51
Ileus dinamic secundar
48
5,37
4
3,31
p=0,3209*
52
5,12
p†
p<0,0001**
Total
894
121
1,015
DMS
5,11±0,60
6,80±0,72
p<0,0001***
5,29±0,66
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
** Chi-square test
*** Comparison of means test
Tabel X. Distribu ia pacien ilor cu abdomen acut hemoragic în func ie de leziunea primară
Nondiabetici
Diabetici
Total
p†
Nr.
%
Nr.
%
Nr.
%
Traumatisme
95
66,90
17
77,27
p=0,5727*
112
68,29
• splenice
42
29,58
8
36,36
p=0,9704*
50
30,49
• hepatice
17
11,97
3
13,64
p=0,4059*
20
12,20
• mezenter
12
8,45
3
13,64
p=0,4082*
15
9,15
• asociate
24
16,90
3
13,64
p=0,4960*
27
16,46
Sarcină extrauterină
17
11,97
2
9,09
p=0,2963*
19
11,59
Chiste ovariene rupte
28
19,72
2
9,09
p=0,5738*
30
18,29
Altele
2
1,41
1
4,55
p=0,0002*
3
1,83
p†
p<0,0001**
Total
142
22
164
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
** Chi-square test
Abdomenul acut hemoragic
Torsiunea de organ
Majoritatea cazurilor de abdomen acut hemoragic
Majoritatea organelor torsionate au fost anexele genitale
au fost generate de traumatisme (68,29%). Chistele
feminine (42,86%), urmate de volvulus sigmoid (37,14%) şi
ovariene rupte şi sarcina extrauterină au reprezentat
volvulus de intestin sub ire, fără diferen ă semni cativă
18,29%, respectiv
11,59% din cazuri, cu diferen ă
statistic
(Tabel XII). Cea mai frecventă interven ie a fost
semni cativă statistic (p<0,0001) (Tabel X).
anexectomia
(46,88%), urmată de rezec ia de sigmoid
Din totalul celor
164 cazuri de abdomen acut
(34,38%), cu diferen ă semni cativă statistic (p=0,0573). Nu
hemorgic, 128 cazuri (78,05%) au fost supuse interven iei
au existat diferen e semni cative între diabetici şi nondiabetici
chirurgicale, procent nesemni cativ mai mare la
în ceea ce priveşte tipul interven iei chirurgicale (p>0,05).
nondiabetici fa ă de diabetici (p=0,8172) (Tabel XI). Cei
Abdomen acut vascular (infarctul enteromezenteric)
mai mul i pacien i au fost supuşi splenectomiei (39,06%),
Abdomenul acut vascular a fost mai frecvent la
procent urmat de anexectomii şi salpingectomii (17,97%,
diabetici decât la nondiabetici
(4,10% vs.
0,96%,
respectiv
14,84%), cu diferen ă semni cativă statistic
p<0,0001). Majoritatea cazurilor au avut infarct de
(p<0,0001) (Tabel XI). Enterectomiile şi hemostaza de
segment de intestin sub ire (37,04%), urmat de intestin
epiplon au fost semni cativ mai frecvente la pacien ii
sub ire total şi intestin sub ire şi gros,
22,22% din
diabetici (5,88% vs, 4,50%, p=0,0117, respectiv 5,88%
cazuri. Localizarea doar la nivelul intestinului gros a fost
vs. 1,80%, p=0,0009).
prezentă la 18,52% din cazuri (Tabel XIII).
110
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Tabelul nr. XI. Interven iile chirurgicale efectuate în abdomenul acut hemoragic
Nondiabetici
Diabetici
Total
p†
Nr.
%
Nr.
%
Nr.
%
Splenectomie
42
37,84
8
47,06
p=0,9248*
50
39,06
Hepatora e
15
13,51
3
17,65
p=0,4725*
18
14,06
Rezec ie hepatică atipică
2
1,80
-
-
2
1,56
Enterectomii
5
4,50
1
5,88
p=0,0117*
6
4,69
Hemostază epiplon
2
1,80
1
5,88
p=0,0009*
3
2,34
Salpingectomii
17
15,32
2
11,76
p=0,3603*
19
14,84
Anexectomii
21
18,92
2
11,76
p=0,4797*
23
17,97
Chistectomie ovariană
7
6,31
-
-
7
5,47
p†
p<0,0001**
Total
111
78,17
17
77,27
p=0,8172*
128
78,05
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
** Chi-square test
Tabel XII. Distribu ia pacien ilor cu torsiune de organ în func ie de cauze
Nondiabetici
Diabetici
Total
p†
Nr.
%
Nr.
%
Nr.
%
Volvulus sigmoid
11
39,29
2
28,57
p=0,6132*
13
37,14
Torsiune anexă (TU, chist)
12
42,86
3
42,86
p=0,5143*
15
42,86
Volvulus intestin sub ire
5
17,86
2
28,57
p=0,4754*
7
20,00
p†
p=0,1077**
Total
28
7
35
Interven iile chirurgicale în abdomenul acut-torsiune de organ
Enterectomii
4
16,00
2
28,57
p=0,4733*
6
18,75
Anexectomii
12
48,00
3
42,86
p=0,6262*
15
46,88
Rezec ie de sigmoid
9
36,00
2
28,57
p=0,5342*
11
34,38
p†
p=0,0573**
Total
25
89,29
7
100
p=0,8172*
32
91,43
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Comparison of proportions
** Chi-square test
Tabel XIII. Distribu ia pacien ilor în func ie de întinderea leziunii de infarct enteromezenteric
Nondiabetici
Diabetici
Total
p†
Nr.
%
Nr.
%
Nr.
%
Intestin sub ire total
10
29,41
2
10,00
p=0,174083*
12
22,22
Segment intestin sub ire
8
23,53
12
60,00
p=0,010013*
20
37,04
Intestin gros
6
17,65
4
20,00
p=1,000000*
10
18,52
Intestin sub ire + gros
10
29,41
2
10,00
p=0,174083*
12
22,22
p†
p=0,1203**
Total
34
0,96%
20
4,1%
54
Interven iile chirurgicale în abdomenul acut torsiune de organ
Enterectomii
8
23,53
12
60,00
p=0,010013* 20
37,04
Colectomie
6
17,65
4
20,00
p=1,000000*
10
18,52
Laparotomie exploratorie
20
58,82
4
20,00
p=0,009911* 24
44,44
p†
p=0,0131**
Total
34
100
20
100
54
100
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Fisher’s exact test
** Chi-square test
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
111
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabel XIV. Distribu ia pacien ilor în func ie de cauzele și formele morfopatologice ale pancreatitei acute
Nondiabetici
Diabetici
Total
Cauze
p†
Nr.
% Nr.
%
Nr.
%
Biliară
144
56,25
30
57,69
p=0,879197*
174
56,49
Toxică
56
21,88
7
13,46
p=0,191674*
63
20,45
Dismetabolică
38
14,84
12
23,08
p=0,151117*
50
16,23
Altele
18
7,03
3
5,77
p=1,000000*
21
6,82
p†
p<0,0001**
Total
256
7,25
52
10,66
308
Forme morfopatologice
Edematoase
112
43,75
15
28,85
p=0,062976*
127
41,23
Necretico-hemoragice
99
38,67
24
46,15
p=0,352595*
123
39,94
Abcese pancreatice
45
17,58
13
25,00
p=0,242703*
58
18,83
p†
p<0,0001**
Total
256
52
308
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Fisher’s exact test
** Chi-square test
Tabel XV. Distribu ia pacien ilor în func ie de tipul de urgen ă în pancreatita acută
Nondiabetici
Diabetici
Total
Tip de urgen ă
p†
Nr.
% Nr.
%
Nr.
%
Urgen ă imediată
20
7,81
15
28,85
p=0,000543*
35
11,36
Urgen ă amânată
42
16,41
8
15,38
p=0,537962*
50
16,23
Urgen ă întârziată
91
35,55
14
26,92
p=0,026192*
105
34,09
p†
p<0,0001**
Total
153
59,77
37
71,15
190
61,69
Tip de urgen ă operată
Urgen ă imediată
20
13,07
14
43,75
p=0,000195*
34
18,38
Urgen ă amânată
42
27,45
6
18,75
p=0,379246*
48
25,95
Urgen ă întârziată
91
59,48
12
37,50
p=0,030772*
103
55,68
p†
p<0,0001**
Total
153
100
32
100
185
100
Interven iile chirurgicale în abdomenul acut pentru pancreatită
Colecistectomie
42
27,45
11
34,38
p=0,847992*
53
28,65
Colecistectomie laparoscopică
82
53,59
12
37,50
p=0,001230*
94
50,81
Colecistectomie+DBE***
18
11,76
7
21,88
p=0,293086*
25
13,51
Necrozectomie
40
26,14
10
31,25
p=1,000000*
50
27,03
Splenectomie
3
1,96
1
3,13
p=1,000000*
4
2,16
Drenaje, lavaje peritoneale
24
15,69
10
31,25
p=0,164041*
34
18,38
Enterectomii
2
1,31
1
3,13
p=0,485067*
3
1,62
p†
p<0,0001**
Total
211
82,42
52
100,00
263
85,39
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* Fisher’s exact test
** Chi-square test
*** DBE- drenaj biliar extern
Toate cazurile de abdomen acut vascular au fost supuse
efectuat enterectomie, procent semni cativ mai mare decât
interven iilor chirurgicale. Laparotomia exploratorie s-a
la nondiabetici (23,53%) (p=0,010013). Colectomiile s-au
efectuat la 44,44% dintre cazuri, enterectomii la 37,04% şi
efectuat în procent nesemnifcativ mai mare la diabetici
colectomii la 18,52%, cu diferen ă statistică (p=0,0131)
(20,00% vs.
17,65%)
(p=1,000000), iar laparatomia
(Tabel XIII). La
60,00% dintre pacien ii diabetici s-a exploratorie s-a efectuat la aproape 3 ori mai mul i pacien i
112
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
nondiabetici decât diabetici
(58,82% vs.
20,00%)
mixtă (ADO + insulină). Remarcăm procentul important
(p=0,009911) (Tabel XIII).
al pacien ilor diagnostica i cu diabet zaharat la internare
Pancreatita acută
(16,39%). După cum era de așteptat, studiul paraclinic
Pancreatita acută a reprezentat 7,66% (308 pacien i)
demonstrează că nivelul gicemiei măsurat înainte de
din totalul cazurilor de abdomen acut, ind mai
interven ia chirurgicală, în prima zi postoperator și în
frecventă la diabetici
10,66% (52 pacien i), fa ă de
timpul spitalizării ulterioare, a fost mai mare la pacien ii
nondiabetici 7,25% (256 pacien i) (p=0,0103).
diabetici decât la cei nondiabetici, cu diferen ă semni cativă
Majoritatea cazurilor de pancreatită acută au fost de
statistic (p<0,0001). În întreaga cohortă, cea mai frecventă
origine biliară (56,49%), cea toxică şi dismetabolică au
formă de abdomen acut a fost cea peritonitică (60,03%),
reprezentat
20,45%, respectiv
16,23%, cu diferen ă
urmată de cea ocluzivă
(25,24%). În timp ce forma
semni cativă
(p<0,0001). Pacien ii nondiabetici au
vasculară, pancreatita acută şi falsul abdomen acut au fost
dezvoltat pancreatită edematoasă cu diferen ă
semni cativ mai frecvente la pacien ii diabetici (p<0,05),
semni cativă fa ă de pacien ii diabetici, în timp ce la
forma peritonitică a fost mai frecventă la nondiabetici
pacien ii diabetici au predominat pancreatita necrotico-
(p=0,0003). În ceea ce privește forma ocluzivă, hemoragică
hemoragică sau abcesul pancreatic, fără semni ca ie
şi torsiunea de organ nu au existat diferen e semni cative
statistică între loturi (Tabel XIV).
statistic între cele două loturi
(p>0,05). Gradul de
Gradul de operabilitate a predominat în cazul
operabilitate a fost nesemni cativ statistic mai mare la
urgen elor întârziate (55,68%). Pacien ii diabetici au avut
nondiabetici fa ă de diabetici
(p>0,05). Morbiditatea
un grad de operabilitate mai mare pentru urgen a imediată
postoperatorie a fost prezentă la 15,06% dintre pacien i, cele
(43,75% vs. 13,07%, p=0,000195), fa ă de nondiabetici,
mai frecvente complica ii postoperatorii ind supura iile de
la care gradul de operabilitate a fost mai mare pentru
plagă şi hematom
(12,58%), urmate de stulele
urgen a întârziată
(59,48% vs. 37,50%, p=0,030772)
postoperatorii la 2,48% din cazuri (p<0,0001). Morbiditatea
Colecistectomia laparoscopică a predominat (50,81%),
generală a fost prezentă la 22,01% pacien i și s-a caracterizat
urmată de colecistectomie
(28,65%), necrozectomie
prin prezen a pneumoniei, a complica iilor cardiovasculare,
(27,03%), drenaje, lavaje peritoneale
(18,38%),
insu cien ei renale acute, infec iei de tract urinar, stărilor
colecistectomie + drenaj biliar extern (DBE) (13,51%),
septice,
dezechilibrului metabolic și tulburărilor
splenectomie (2,16%) și enterecomii (1,62%), cu diferen ă
neurologice, cu semni ca ie statistică între variabile
semni cativă statistic (p<0,0001) (Tabel XV).
(p<0,0001). În studiul de fa ă, prezen a morbidită ii a
Atât la nondiabetici, cât şi la diabetici, cea mai
prelungit durata medie de spitalizare cu aproximativ 2 zile la
ridicată mortalitate s-a înregistrat în cazul formei
pacien ii nondiabetici și cu 10,2 zile la pacien ii diabetici,
vasculare
(11,76%, respectiv
25,00%), urmată de
precum și sta ionarea în sec ia ATI, cu diferen ă semni cativă
peritonită
(5,65% vs.
10,94; RR=1,0593/p=0,0105)
statistic între cele două loturi (p<0,0001). În lotul nostru de
pancreatita acută (8,59%, respectiv 11,54%). Indiferent
studiu s-au înregistrat 238 decese, rezultând o mortalitate
de forma abdomenului acut mortalitatea a fost mai mare
generală de 5,92%, semni cativ mai mare la diabetici, decât
la diabetici fa ă de nondiabetici.
la nondiabetici (9,84% vs. 5,38%) (p=0,0018). În general,
bărba ii au avut un risc crescut de mortalitate fa ă de femei.
Discuții
Riscul de deces la femeile diabetice a fost mai mare decât la
femeile nondiabetice (RR=1,0585/p=0,0047). Prin urmare,
În studiul nostru, majoritatea pacien ilor au fost de sex
pacien ii diabetici, de sex feminin, proveni i din mediul
feminin, atât la nondiabetici, cât și la diabetici, rezultând
urban, cu vârsta peste
50 ani, datorită prezen ei
un raport F/M de 1,6:1, respectiv 1,4:1, cu diferen ă
hiperglicemiei peri-, intra- și post-operatorii au avut un risc
semni cativă statistic (p<0,0001). Vârsta medie la diabetici
crescut pentru complica ii postoperatorii, atât locale cât și
a fost semni cativ mai mare decât la nondiabetici (62,14
generale, acestea crescând riscul mortalită ii postoperatorii,
ani vs. 49,37 ani) (p<0,0001). Peste 60% din pacien ii
comparativ cu pacien ii nondiabetici. Mortalitatea maximă
nondiabetici au avut vârste cuprinse între 30-69 ani, în
s-a înregistrat în cazul pacien ilor cu formă vasculară de
timp ce în lotul pacien ilor diabetici cu abdomen acut
abdomen acut (16,67%), urmată de pancreatita acută
majoritatea (85,86%) au avut vârste peste 50 ani. Studiul
(9,09%), abdomenul acut hemoragic (6,71%) şi peritonitic
clinic arată că majoritatea pacien ilor diabetici cu abdomen
(6,21%). Nu s-au înregistrat decese în cazul torsiunii de
acut au avut diabet zaharat tip II (95,90%) (p<0,0001) cu
organ.
o durată de evolu ie a diabetului de peste 10 ani (34,43%),
La pacien ii diabetici prezen a morbidită ii
trata i cu antidiabetice orale (57,79%). Insulinodependen ii
postoperatorie s-a înregistrat la 36,27% dintre pacien ii
au reprezentat 25,82%, din care 15,16% au urmat terapie
opera i, procent semni cativ mai mare decât la pacien ii
A Comparative Case Study of Acute Abdomen in Diabetic and Non-Diabetic Patients
113
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
nondiabetici (14,43%) (p<0,0001). Riscul relativ este
Diabetes in older adults: a consensus report. J Am
semni cativ diferit de 1, prin urmare există un risc crescut
Geriatr Soc 2012;60(12):234256.
de apari ie a morbidită ii postoperatorii la pacien ii
3.
American Diabetes Association. Standards of medical
diabetici fa ă de nondiabetici pentru supura ii la nivelul
care in diabetes-2012. Diabetes Care 2012;35 Suppl
plăgii postoperatorii, hematom și stule intestinale. În
1:S11-63.
ceea ce privește morbiditatea generală, remarcăm un risc
4.
Inzucchi SE, Bergenstal RM, et al. Management of
crescut pentru sepsis, dezechilibru metabolic, pneumonie,
hyperglycaemia in type 2 diabetes: a patient-centered
infec ie de tract urinar, insu cien ă renală acută și
approach. Diabetologia 2012;55(6):1577-96.
complica ii cardiovasculare la pacien ii diabetici,
5.
Noordzij PG, Boersma E, Schreiner F, et al. Increased
comparativ cu cei nondiabetici (p<0,05).
preoperative glucose levels are associated with perioperative
Se estimează că
25% dintre pacien ii cu diabet
mortality in patients undergoing noncardiac, nonvascular
zaharat vor necesita interven ie chirurgicală [9]. Rata
surgery. Eur J Endocrinol 2007;156:137-142.
mortalită ii la pacien ii cu diabet zaharat a fost estimată a
6.
Krentz AJ, Nattras M. Acute metabolic complications of
de până la 5 ori mai mare decât la pacien ii nediabetici,
diabetes. In: Pickup JC, William G. Textbook of
datorată insu cien ei multiple de organe
[10].
diabetes. Black well Science Ltd 2003, 32.10-32.22.
Complica iile cronice care rezultă din microangiopatie
7.
Pătrașcu T, Doran H, Catrina E, et al. Particularită i
(retinopatie, nefropatie și neuropatie) și macroangiopatie
ale chirurgiei la diabetici, Ed. Niculescu, 2005.
(ateroscleroză) cresc în mod direct necesitatea unei
8.
Păcescu E, Bugă C, Pătrașcu T, Brezean I, Doran H.
interven ii chirurgicale și apari ia complica iilor
Di cultă i de diagnostic în abdomenul acut peritonitic
chirurgicale din cauza infec iilor și vasculopatiilor [11].
la bolnavul diabetic, Chirurgia 1999;6(94):485-93.
Infec iile reprezintă
66% din complica iile
9.
Blomgren KB, Sundström A, Steineck G, Wiholm
postoperatorii și aproape un sfert din decesele
BE. Obesity and treatment of diabetes with glyburide
perioperatorii la pacien ii cu DZ. Datele sugerează
may both be risk factors for acute pancreatitis. Diabetes
afectarea func iei leucocitare, inclusiv modi carea
Care 2002;25(2):298-302.
chemotaxiei și activitatea fagocitară [12]. Dezvoltarea
10.
Smiley DD, Umpierrez GE. Perioperative glucose
hiperglicemiei perioperatorii s-a dovedit a un predictor
control in the diabetic or nondiabetic patient, South
sensibil al infec iei nozocomiale în studii observa ionale
Med J 2006;99:580-589; quiz 590-591.
mici în chirurgia generală. Un control strict al glicemiei
11.
Umpierrez GE, Isaacs SD, Bazargan N, You X, aler
este important pentru a minimiza infec ia [13].
LM, Kitabchi AE. Hyperglycemia: an independent
În plus fa ă de complica iile infec ioase
marker of in-hospital mortality in patients with
postoperatorii, ischemia miocardică postoperatorie este
undiagnosed diabetes. J Clin Endocrinol Metab
crescută în rândul pacien ilor cu DZ supuși unei
2002;87:978-982.
interven ii chirurgicale cardiace și noncardiace
[14].
12.
Ramos M, Khalpey Z, Lipsitz S, et al. Relationship of
Date din studiile observa ionale sugerează că la pacien ii
perioperative hyperglycemia and postoperative infections
chirurgicali, cu și fără diabet zaharat, controlul strict al
in patients who undergo general and vascular surgery.
glicemiei afectează pozitiv morbiditatea și mortalitatea
Ann Surg 2008;248:585-59116.
într-o varietate de popula ii chirurgicale [15,16]. Cu
13.
Bailey IS, Rhodes M, O’Rourke N, Nathanson L,
toate că un control glicemic intensiv continuă să e
Fielding G. Laparoscopic management of acute small
standardul de îngrijire a pacientului diabetic, există
bowel obstruction. Br J Surg 1998;85(1):84-7.
riscul unei hipoglicemii secundare contrar bene ciului
14.
Dragomirescu C, Li escu M, Iordache N, et al.
adus în morbiditate și mortalitate. Scopul este de a găsi
Conversions and reinterventions in laparoscopic
un echilibru în această situa ie, motiv pentru care
cholecystectomy. Chirurgia 1998;93(5):279-84.
orientarile actuale recomandă un control glicemic mai
15.
Pant N, Kadaria D, Murillo LC, Yataco JC, Headley
pu in strict, de obicei, între 80-150 mg/dL [17].
AS, Freire AX. Abdominal Pathology in Patients With
Diabetes Ketoacidosis. Am J Med Sci 2012 Jan 20.
References
16.
Haap M, Artunc F, Haa CS, Horger M, Teichmann R,
Riessen R. A rare di erential diagnosis of acute abdominal
1. Krinsley JS. E ect of an intensive glucose management
pain. Dtsch Med Wochenschr 2009;134:28-29.
protocol on the mortality of critically ill adult patients.
17.
Kimura W, Mizutani M, Fuse A. Problems and
Mayo Clin Proc 2004;79(8):992-1000.
therapeutic strategy for emergency operation of the
2. Sue Kirkman M, Briscoe VJ, Clark N, et al.
abdomen in the aged. Nihon Ronen Igakkai Zasshi
Development Conference on Diabetes and Older Adults.
2004;41(6):660-5.
114
Dejeu et al
ORIGINAL ARTICLES
ACTUALITĂȚI ÎN TRATAMENTUL CHISTULUI HIDATIC HEPATIC
Adela Camelia Nichita1, Adrian Maghiar2, Daniela Dinulescu3, Teodor Traian Maghiar4
1Sec ia Radiologie - Imagistică medicală, Spitalul Municipal „Dr. Pop Mircea” Marghita, 2Sec ia Chirurgie generală,
Departament Discipline Chirurgicale, 3Sec ia Radiologie - imagistică medicală, Departament Discipline Morfologice,
4Departament Discipline Morfologice, Spitalul Pelican Oradea a liat Facultă ii de Medicină și Farmacie Oradea,
România
Adresa pentru coresponden ă:
Dr. Adela Camelia Nichita
Facultatea de Medicină și Farmacie Oradea, România
Pia a 1 Decembrie 10, 410073, Oradea, Romania
Tel: +40744400774
Email: adela_abrudan@yahoo.com
Primit: 05.08.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 115-122
Rezumat
Rezultate: Dintre cei 120 pacien i, 74 au fost femei,
iar 46 au fost bărba i, 48 au provenit din mediul urban,
Studiul de fa ă face o analiză a tratamentului
iar 72 din mediul rural, inciden a maximă a bolii ind la
modern al chistului hidatic hepatic, cu scopul selectării
grupa de vârstă 31-40 ani, urmată de 41-50 ani (p<0,05).
terapiei adecvate pentru o morbiditate, mortalitate şi
Comparând cele două loturi de pacien i din punct de
recuren ă cât mai mici pentru boala hidatică a catului.
vedere al procedurilor chirurgicale, perichistectomia
Material și metode: Studiul s-a realizat pe un număr
par ială Lagrot s-a practicat pacien ilor trata i
de 120 pacien i interna i cu diagnosticul de chist hidatic
laparoscopic
(p=0,0010), iar lobectomia stângă s-a
hepatic. S-a urmărit inciden a bolii hidatice hepatice în
practicat pacien ilor trata i chirurgical clasic (p=0,0468).
func ie de vârstă, sex, mediul de provenien ă, evaluarea
Din punct de vedere al evolu iei postoperatorii, rata
clinică și paraclinică, precum și tratamentul instituit:
morbidită ii și recuren a bolii au fost mai mari la pacien ii
medical, chirurgical clasic
(radical sau conservator) şi
trata i chirurgical conservator, aceștia prezentând un risc
laparoscopic. Pacien ii asimptomatici (20) au bene ciat de
crescut pentru stula biliară externă, fa ă de cei trata i
tratament medicamentos, iar cei simptomatici (100), de
chirugical radical și laparoscopic. Decesul a survenit la
tratament chirurgical și medicamentos. Aceștia au fost
patru dintre pacien ii trata i chirurgical clasic, datorită
grupa i în două loturi: Lotul A - 78 (78%) pacien i eligibili
complica iilor
postoperatorii
generale,
emboliei
pentru tratamentul chirurgical clasic, dintre care
38
pulmonare şi stării septice cu insu cien ă multiplă de
(48,72%) supuşi unei interven ii chirurgicale conservatoare
organe. Complica iile au condus la creşterea perioadei de
şi 40 (51,28%) supuşi unei interven ii chirurgicale radicale
spitalizare a pacientului la
60 zile. Coe cientul de
și Lotul B - 22 (22%) pacien i eligibili pentru tratamentul
corela ie între tratamentul chirurgical clasic şi
laparoscopic (chist necomplicat, de dimensiuni mijlocii,
laparoscopic şi apari ia stulei biliare externe, ca şi
corticalizat şi localizat în segmentele anterioare hepatice
complica ie comună postoperator, arată o corela ie
(segmentele II - VI după clasi carea lui Couinaud).
moderată între variabilele respective.
News in the Treatment of Hepatic Hydatid Cyst
115
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Concluzii: Rata morbidită ii și recuren a bolii au
Oradea, Clinica de Chirurgie a Spitalului Pelican
fost mai mari la pacien ii cărora li s-a practicat o
Oradea și Clinica de Radiologie a Spitalului Clinic
interven ie chirurgicală care păstrează par ial sau total
Jude ean de Urgen ă Oradea.
perichistul, aceștia prezentând un risc crescut pentru
Dintre cei 120 de pacien i, 20 au fost asimptomatici,
stula biliară externă. Abordul laparoscopic oferă o
bene ciind de tratament medicamentos, iar 100 au avut
alternativă viabilă la chirurgia clasică pentru tratamentul
chist hidatic hepatic simptomatic, unde tratamentul a
chisturilor hidatice hepatice și este demn de a luat în
fost chirurgical și medicamentos. Aceștia au fost grupa i
considerare pentru situa ii adecvate. Studiul de fa ă
în două loturi: Lotul A - 78 (78%) pacien i eligibili
demonstrează existen a unei corela ii moderate între
pentru tratamentul chirurgical clasic, dintre care
38
apari ia stulei biliare externe, ca şi complica ie comună
(48,72%) au fost supuşi unei interven ii chirurgicale
postoperator și tratamentul chirurgical clasic
conservatoare (interven ie care păstrează par ial sau total
(conservator, radical) şi laparoscopic.
perichistul) şi
40 (51,28%) supuşi unei interven ii
Cuvinte cheie: chist hidatic hepatic, tratamentul
chirurgicale radicale
(interven ie care excizează în
chirurgical,
perichistectomie
par ială
Lagrot,
totalitate perichistul) și Lotul B - 22 (22%) pacien i
perichistectomie totală, hepatoctomie
eligibili
pentru tratamentul laparoscopic
(chist
necomplicat, de dimensiuni mijlocii, corticalizat şi
Introducere
localizat în segmentele anterioare hepatice (segmentele
II-VI după clasi carea lui Couinaud).
Chisturile hidatice netratate cresc în dimensiune și
Consim ământul informat a fost dat de to i
în cele din urmă provoacă complica ii care duc la
pacien ii, iar studiul a fost aprobat de comisia de avizare
invaliditate sau chiar exitus. Numai în cazuri
internă a lucrărilor de cercetare-dezvoltare din cadrul
excep ionale se poate produce vindecarea spontană prin
spitalului.
moartea parazitului și calci erea chistului. Din aceste
Pentru abordul chirurgical deschis, s-a realizat o
motive, este general acceptat faptul că boala hidatică
incizie mediană supraombilical sau o incizie subcostală.
hepatică diagnosticată la timp trebuie tratată cât mai
Orice adeziune între chist și organele vecine a fost lizată.
precoce [1].
Pentru a preveni hidatidoza peritoneală secundară,
Nu există încă un consens cu privire la forma
cavitatea peritoneală a fost izolată cu meşe îmbibate în
optimă de tratament. Tratamentul modern al chistului
solu ie salină hipertonă 20% înainte de orice manevră
hidatic hepatic variază de la interven ie chirurgicală, la
efectuată pe chistului hidatic. Inactivarea parazitului a
drenaj percutan sau terapie medicală.
fost realizată prin injectarea de solu ie salină hipertonă
Studiul de fa ă face o analiză a tratamentului
20%. După 5 minute, con inutul hidatic a fost aspirat.
modern al chistului hidatic hepatic, cu scopul selectării
Pornind de la locul de injectare, s-a efectuat chistotomia,
terapiei celei mai adecvate pentru a ob ine o morbiditate,
cu extragerea membranei germinale și a veziculelor ice.
mortalitate şi recuren ă cât mai mici. Acest deziderat se
În studiul de fa ă s-a efectuat perichistectomie
realizează în contextul unei experien e clinice de cinci
totală, lobectomie stângă şi hepatectomie stângă, ca
ani în tratarea chistului hidatic hepatic.
proceduri radicale, perichistectomie par ială Lagrot, ca
Obiectivele au urmărit e cien a comparativă a
procedură conservatoare.
procedurilor chirurgicale radicale versus conservatoare,
Pentru abordul laparoscopic s-au realizat patru
fezabilitatea, siguran a şi e cien a tratamentului
incizii: una supraombilicală de 10 mm prin care s-a
laparoscopic versus tratamentul chirurgical clasic. De
introdus un laparoscop, o altă incizie de 10 mm la
asemenea s-a urmărit rata morbidită ii, mortalită ii şi
nivelul epigastrului, cât mai aproape posibil de chist,
recuren ei bolii, stabilirea unei corela ii între tipul de
ind folosită ca un canal de lucru și două incizii de 5
tratament practicat şi apari ia
stulei
biliare
mm în func ie de localizarea chistului. În cavitatea
postoperatorii, complica ie prezentă în ambele tipuri de
abdominală a fost insu at dioxid de carbon și orice
tratament practicat.
adeziune între chist și organele vecine a fost lezată.
Pentru a împiedica hidatioza secundară prin trocarele de
Material și metode
lucru s-au introdus meşe îmbibate în solu ie salină
hipertonă 20% şi s-a izolat chistul hidatic de restul
Acest studiu s-a desfăşurat în perioada 2007-2013,
cavită ii peritoneale. Apoi cu un ac de punc ie, cu
pe un număr de 120 pacien i interna i cu diagnosticul
diametrul de 5 mm, legat la un sistem de aspira ie, se
de chist hidatic hepatic, ind o colaborare între Clinica
punc ionează chistul hidatic şi se aspiră o parte din
de Chirurgie I a Spitalului Clinic Jude ean de Urgen ă
con inut. O altă canulă de aspira ie este introdusă prin
116
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
alt trocar de lucru şi men inută permanent în apropierea
Tabelul I. Caracteristici demogra ce, clinice, paraclinice şi
acului de punc ie, pentru a preveni orice scurgere a
tratament ale pacien ilor suferind de chist hidatic hepatic
lichidului hidatic. Acul de punc ie, odată introdus în
TOTAL PACIEN I
120
p†
cavitatea chistică, nu mai este extras până la evacuarea
Sex
completă a con inutului chistic. Acest lucru cumulat cu
Feminin
74 (61,7%)
prezen a canulei de aspira ie în vecinătatea acului de
p=0,000466*
Masculin
46 (38,3%)
punc ie şi prezen a meşelor îmbibate cu solu ie scolicidă
Vârsta medie (ani)
(20-30) 14
în jurul chistului împiedică scurgerea con inutului
(31-40) 54
hidatic din interiorul chistului la nivelul cavită ii
p<0,0001**
(41-50) 36
peritoneale, scăzând la minimum posibilitatea de
(51-69) 16
diseminare a lichidului hidatic la nivelul cavită ii
Mediul
peritoneale şi apari iei hidatidozei secundare.
Urban
48 (40%)
Se injectează solu ie salină hipertonă
20% în
p=0,002907*
Rural
72 (60%)
interiorul chistului pentru inactivarea parazitului. După
Tabloul clinic
5 minute, con inutul hidatic a fost aspirat. Pornind de la
Asimptomatici
20 (17%)
locul de injectare, s-a practicat chistotomia şi inspec ia
p<0,000001*
Simptomatici
100 (83%)
cavită ii perichistice cu laparoscopul cu scopul
Chist hidatic complicat
10 (10%)
identi cării eventualelor stule biliochistice. Membrana
p<0,000001*
Chist hidatic necomplicat
90 (90%)
germinală, perichistul sec ionat şi meşele imbibate au
Clasi carea ecogra că chistică£
fost extrase într-o pungă de plastic (endobag).
Asimptomatici
Procedurile chirurgicale alese pentru tratamentul
Tipul I/CE1
4 (20%)
laparoscopic al cavită ii reziduale au fost perichistectomia
p=0,000360*
Tipul II/CE3
16 (80%)
par ială Lagrot
(și drenajul cavită ii rămase) și
Simptomatici
perichistectomie totală.
Tipul II/CE3
6 (6%)
Cu scopul de a preveni o eventuală hidatidoză
Tipul III/CE2
64 (64%) p<0,0001**
secundară prin contaminare intraoperatorie, to i
Tipul IV/CE4
30 (30%)
pacien ii au fost trata i cu albendazol
(10 mg/kg/zi)
Loca ia chisturilor tratate chirurgical după
preoperator 7 zile şi postoperator 3 luni, cu urmărirea
clasi carea lui Couinaud
transaminazelor hepatice.
Segmentele II-IV
30 (30%)
Metodele de analiză statistică au fost testul Chi-
Segmentele V-VI
36 (36%) p=0,6570**
pătrat, Fisher’s exact test, Comparison of means test,
Segmentul VIII
34 (34%)
Comparison of proportions test, Relative risk test şi
Tratament
calcularea coe cientului de corela ie utilizând programul
Chirurgical clasic
78 (78%)
p<0,000001*
de statistică medicală MedCalc® versiunea
12.2.1.0
Laparoscopic
22 (22%)
(MedCalc® Software, Mariakerke, Belgium).
* Fisher’s exact test
** Chi-square test
Rezultate
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile
studiate
£ clasi carea ecogra că Gharbi/Clasi carea ecogra că WHO a
Din cei 120 pacien i interna i cu suspiciunea de
chistului hidatic
chist hidatic hepatic, 74 au fost femei, iar 46 au fost
bărba i, 48 au provenit din mediul urban, iar 72 din
mediul rural, cu diferen ă semni cativă din punct de
radiogra că de rutină (p<0,000001). Inciden a chistului
vedere statistic, p<0,05.
hidatic hepatic complicat la pacien ii lua i în studiu a
Inciden a maximă a bolii a fost în grupa de vârstă
fost de 10% (Tabelul I).
31-40 ani, urmată de 41-50 ani, afectând persoanele
Imagistic, ecogra a abdominală a avut un rol
tinere, care prin natura muncii pe care o practică vin în
deosebit în diagnosticarea chistului hidatic hepatic.
contact cu vectorul bolii (Tabelul I).
Prezen a simptomatologiei este direct propor ională cu
Din punct de vedere clinic, majoritatea pacien ilor
gradul de leziune ecogra că. Astfel, pacien ii
(83%) au prezentat simptomatologie clinică, absen a
asimptomatici, a ându-se într-un stadiu incipient al
tabloului clinic dovedindu-se la pacien ii (17%) a a i
bolii, cu leziuni chistice de Tipul I/CE1 şi Tipul II/CE3,
într-un stadiu incipient al bolii, leziunea chistică ind
au bene ciat de tratament medicamentos cu Albendazol
descoperită accidental la o examinare ecogra că sau
(Zentel)
10 mg/kg/zi trei luni, spre deosebire de
News in the Treatment of Hepatic Hydatid Cyst
117
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
localizarea chistelor hidatice în segmentele II-IV - 10
(26%), segmentele V-VI - 14 (37%), segmentele I-VII
- 10 (26%) și segmentul VIII - 4 (11%) (p=0,0670), și
40 (51,28%) radical, localizarea chistelor hidatice ind
în segmentele II-IV - 12 (30%), segmentele V-VI - 18
(45%), segmentele I-VII - 6 (15%) și segmentul VIII -
4 (10%) (p=0,0011).
Pacien ii Lotului B - 22 (22%) au fost opera i prin
abord laparoscopic. Acesta a fost practicat la pacien ii cu
chist hidatic necomplicat, localizat predominant în
Figura 1. Tratamentul chirurgical în func ie de localizarea
segmentele hepatice V-VI -12 (55%), II-IV - 8 (36%) și
chistului în segmentele hepatice
segmentul VIII -2 (9%) (p=0,0001) (Figura 1).
Chisturile hidatice operate laparoscopic au fost
chisturi tinere Tipul II/CE3 şi Tipul III/CE2,
pacien ii simptomatici unde stadiul evolutiv al leziunilor
necomplicate, localizate predominant în segmentele
chistice a fost mai avansat, predominând Tipul III/CE2
hepatice II-VI marginale, în timp ce tratamentul
în propor ie de 64%, care au bene ciat de tratament
chirurgical clasic a fost practicat la chisturile de Tipul
chirurgical asociat cu tratament medicamentos. Acesta a
III/CE2, urmate de Tipul IV/CE4 (Tabelul II).
constat în proceduri chirurgicale clasice conservatoare
Stadiul CE2 WHO (World Health Organization)
(Perichistectomie par ială Lagrot) sau radicale
se caracterizează prin chisturi- ice cu aspect de „fagure
(perichistectomie
totală,
hepatoctomie stângă,
de miere”, care pot umple par ial sau complet chistul
lobectomie stângă) și laparoscopic, în func ie de
mamă unilocular, fertil și are corespondent Tipul III
localizarea şi polimor smul leziunilor.
Gharbi, o colec ie lichidiană cloazonată, dată de un
Analizând distribu ia pacien ilor cu chist hidatic pe
proces de vezicula ie internă declanşată de o agresiune
cele două loturi în func ie de segmenta ia catului,
mecanică, chimică sau infec ioasă a chistului.
putem observa că în lotul A reparti ia chisturilor este
Stadiul CE3 WHO de tranzi ie, se caracterizează
relativ bine propor ionată la pacien ii cu tratament
prin chisturi care degenerează, dar con in încă
chirurgical conservator, fa ă de cei la care s-a practicat
protoscolecşi viabili, membrane plutitoare în lichidul
tratament chirurgical radical. Aici chisturile au avut
chistic şi are corespondent Tipul II Gharbi, o colec ie
localizare în segmentele marginale ale catului, acest
lichidiană +/- nisip hidatic cu perete dedublat și început
lucru permi ând tehnica propriu-zisă şi evitând riscul
de decolare a membranei hidatice (decolare par ială sau
interceptării unor pediculi vasculo-biliari majori.
totală).
În Lotul A
78
(78%) pacien i au fost trata i
Stadiul CE4 WHO corespunde unui chist hidatic
chirurgical clasic,
38
(48,72%) conservator, cu
inactiv, caracterizat printr-o degenerare avansată,
Tabelul nr. II Tratamentul chirurgical în func ie de clasi carea ecogra că Gharbi /WH
și dimensiunea medie a chistului hidatic (cm)
Total pacien i
Lotul A
Lotul B
p†
100 (100%)
78 (78%)
22 (22%)
Tipul II/CE3
0
6 (27%)
p=0,000063*
Tipul III/CE2
48 (62%)
16 (73%)
p=0452202*
Tipul IV/CE4
30 (38%)
0
p=0,000145*
Dimensiunea medie a chistului hidatic (cm)
10,48±4,74 (2-18)
8,36±5,27 (2-15) p=0,0737**
Perichistectomie par ială Lagrot
38 (48,72%)
20 (90,91%)
p=0,0010***
Perichistectomie totală
22 (28,21%)
2 (9,09%)
p=0,1160***
Lobectomie stângă
16 (20,51)
0
p=0,0468***
Hepatectomie stângă
2 (2,56%)
0
p=0,9166***
* Fisher’s exact test
** Comparison of means test
*** Comparison of proportions test
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
£ clasi carea ecogra că Gharbi / Clasi carea ecogra că WHO a chistului hidatic
118
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
48,72% care arată o diferen ă semni cativă statistic
(p=0,0010) și lobectomiei stângi efectuată la 20,51%
din pacien ii trata i chirurgical clasic, fa ă de cei trata i
laparoscopic (p=0,0468) (Tabelul II; Figura 2).
Din punct de vedere al evolu iei postoperatorii,
putem observa că rata morbidită ii a fost semni cativ
mai mare în rândul pacien ilor trata i chirurgical clasic,
fa ă de cei trata i laparoscopic (complica ii chirurgicale
82% vs. 18%, p<0,0001 / complica ii generale 37% vs.
0, p=0,0018), analiza statistică arătând o inciden ă
crescută a complica iilor la nivelul plăgilor (seroame şi
Figura 2. Distribu ia pacien ilor în func ie de procedurile
abcese), urmate de stula biliară externă, abces al
chirurgicale
cavită ii reziduale şi hemoragie (Tabelul III).
Decesul a survenit la patru dintre pacien ii trata i
chirurgical clasic, datorită complica iilor postoperatorii
probabil infertil, cu aspect eterogen, cu pu ine sau fără
generale, emboliei pulmonare și stării septice cu
chisturi- ice, având corespondent Tipul IV Gharbi -
insu cien ă multiplă de organe. Aceste complica ii au
forma iune cu ecostructură solidă, aspect heterogen,
condus la creşterea perioadei de spitalizare a pacientului
corespunzând unui chist remaniat, îmbătrânit.
la 60 zile, statistic semni cativ (p<0,0001) comparativ
Chisturile hidatice tratate chirurgical clasic au avut
cu lotul pacien ilor trata i laparoscopic (Tabelul III).
dimensiuni cuprinse între
2-18 cm, cu o medie de
Supravegherea periodică la 3, 6 şi 12 luni postoperator,
10,48±4,74 fără diferen ă semni cativă statistic fa ă de
clinică şi imagistică, nu a înregistrat recidive ale bolii
cele tratate laparoscopic, unde dimensiunile au variat
hidatice la pacien ii trata i laparoscopic, spre deosebire
între 2-15, cu o medie de 8,36±5,27 (Tabelul II).
de pacien ii trata i chirurgical clasic, a căror rată de
Făcând o compara ie între procedurile chirurgicale,
recidivă a bolii a fost de 5% (Tabelul III; Figura 3).
rezultatele au fost similare între cele două loturi de
Analizând e cien a comparativă a procedurilor
studiu, cu excep ia perichistectomiei par iale Lagrot
chirurgicale radicale versus conservatoare
(interven ie
efectuată la 90,91% din pacien ii trata i laparoscopic,
care păstrează par ial sau total perichistul) în ceea ce
comparativ cu cei trata i chirurgical clasic în procent de
priveşte rata morbidită ii şi recuren a bolii, studiul de
Tabelul III. Morbiditatea şi mortalitatea postoperatorie la pacien ii opera i
pentru chist hidatic hepatic
Total pacien i
Lotul A
Lotul B
p†
100 (100%)
78 (78%)
22 (22%)
Complica ii chirurgicale
p<0,0001*
Complica iile plăgilor
30 (38%)
0
p=0,0015*
Fistulă biliară externă
24 (31%)
2 (9%)
p=0,0720*
Abces al cavită ii reziduale
4 (5%)
2 (9%)
p=0,8483*
Hemoragie
6 (8%)
0
p=0,3837*
Complica ii generale
p=0,0018*
Pneumonie
10 (13%)
0
p=0,1663*
Efuziuni pleurale
14 (18%)
0
p=0,0720*
Embolie pulmonară
2 (3%)
0
p=0,9811*
Insu cien ă multiplă de organe
2 (3%)
0
p=0,9811*
Recidivă
4 (5%)
0
p=0,6553*
Mortalitate
4 (5%)
0
p=0,6553*
Timpul operator (minute)
82,46±23,79
87,63±26,73
p=0,3832**
(35-120)
(40-140)
Zile de spitalizare
32,53±16,14
11,63±2,73
p<0,0001**
(7-60)
(7-16)
* Comparison of proportions test
** Comparison of means test
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
News in the Treatment of Hepatic Hydatid Cyst
119
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabelul IV. Morbiditatea şi recuren a bolii postoperator
Interven ii
Interven ii
Lotul A
Risc relativ
conservatoare
radicale
p†
78 (78%)
(IC 95%)
38 (48,72%)
40 (51,28%)
Morbiditatea
p=0,0016*
Hemoragie
2 (5%)
4 (10%)
1,0526
p=0,4308**
(0,9265-1,1959)
Fistulă biliară externă
20 (53%)
4 (10%)
0,5263
p=0,0003**
(0,3706-0,7474)
Abces al cavită ii reziduale / subfrenic
2 (5%)
2 (5%)
0,9972
p=0,9580**
(0,8994-1,10581)
Recidivă
4 (11%)
0
0,8955
p=0,0676**
(0,7956-1,008)
* Comparison of proportions test
** Relative risk test
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
fa ă demonstreză că rata morbidită ii a fost mai mare la
pacien ii care au bene ciat de interven ii conservatoare
(p=0,0016), cu un risc crescut semni cativ statistic
pentru stula biliară externă
(p=0,0003), ca şi rata
recuren ei bolii, însă fără diferen ă semni cativă statistic
între cele două loturi
(Tabelul IV; Figura
4).
Complica iile hemoragice au fost mai frecvente la
pacien ii trata i chirurgical radical, însă fără diferen ă
semni cativă fa ă de cei trata i chirurgical conservator.
Doi pacien i trata i chirurgical conservator au avut
Figura 3. Rata de recidivă a bolii hidatice postoperator
abces al cavită ii reziduale, iar al i doi trata i chirurgical
la cele două loturi de pacien i lua i în studiu
radical au avut abces subfrenic (Tabelul IV).
Fistula biliară externă a fost o complica ie
postoperatorie în
20 de cazuri tratate chirurgical
conservator
(din totalul de
38), în
4 cazuri tratate
chirurgical radical (din totalul de 40) și în 2 cazuri din
cele 22 operate laparoscopic.
Coe cientul de corela ie între tratamentul
chirurgical conservator, radical şi laparoscopic şi apari ia
stulei biliare externe, ca şi complica ie comună
postoperator (r=0,5), arată o corela ie moderată între
variabilele respective (Figura 5).
Figura 4. Rata de recidivă a bolii hidatice postoperator
este mai mare la pacien ii trata i chirurgical conservator
Discuții
Un management terapeutic optim al pacientului cu
boală hidatică hepatică înseamnă o evaluare atentă,
luând în considerare localizarea şi numărul chisturilor
hidatice, prezen a complica iilor, în special biliare,
riscurile și bene ciile, indica iile și contraindica iile,
experien a chirurgului, înainte de a lua o decizie cu
privire la tipul interven iei chirurgicale și momentul
efectuării acesteia [2,3].
Chirurgia rămâne terapia standard de aur [4,5] și
poate
efectuată clasic sau prin abord laparoscopic.
Figura 5. Corela ia între tipul de tratament chirurgical
şi apari ia stulei biliare postoperatorii
Procedurile chirurgicale efectuate pentru chisturi
120
Nichita et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
hidatice pot împăr ite pe scurt în abordări radicale și
sigur şi e cient pentru tratarea pacien ilor cu chist
conservatoare.
Procedurile
radicale
includ
hidatic necomplicat, de dimensiuni mijlocii, corticalizat
perichistectomia și rezec ia hepatică. Cu toate acestea,
şi localizat de preferin ă în segmentele anterioare hepatice
tehnica cea mai comună este chistectomia totală sau
(segmentele II-VI după clasi carea lui Couinaud). Luând
par ială [6-9].
în considerare binecunoscutele bene cii ale chirurgiei
Aceste proceduri chirurgicale pot
înso ite de
minim invazive, abordul laparoscopic oferă o alternativă
reac ii alergice sau ana lactice, precum şi de riscul
viabilă la chirurgia clasică pentru tratamentul chisturilor
diseminării secundare, de aceea se indică chimioterapia
hidatice hepatice și este demn de a luat în considerare
cu mebendazol sau albendazol înainte și mai ales după
pentru situa ii adecvate.
interven ia chirurgicală. Tratamentul cu albendazol pare
În ceea ce privește apari ia stulei biliare externe, ca
a
mai e cient datorită penetrării și absorb iei mai
şi complica ie comună postoperator, studiul de fa ă
bune. Gil Grande și colab. au arătat ca albendazolul (10
demonstrează existen a unei corela ii moderate între
mg/kg/zi) sterilizează chistul în 72% din cazuri după
această complica ie și tratamentul chirurgical clasic
prima lună de tratament și în 94% după 3 luni de
(conservator, radical) şi laparoscopic.
tratament [10,11].
În studiul de fa ă tratamentul chistului hidatic
hepatic a fost medical, chirurgical clasic, conservator
Referințe
(perichistectomie par ială Lagrot) sau radical
(perichistectomie
totală,
hepatoctomie stângă,
1.
Eckert J, Deplazes P. Biological, epidemiological, and
lobectomie stângă) și laparoscopic în func ie de
clinical aspects of echinococcosis, a zoonosis of increasing
localizarea şi polimor smul leziunilor. Analizând
concern. Clin Microbiol Rev 2004;17(1):107-35.
distribu ia pacien ilor cu chist hidatic pe cele două
2.
Magistrelli P, Masetti R, Coppola R, Messia A, Nuzzo
loturi în func ie de segmenta ia catului, în lotul A
G, Picciocchi A. Surgical treatment of hydatid disease of
reparti ia chisturilor a fost relativ bine propor ionată la
the liver. A
20-year experience. Arch Surg
pacien ii cu tratament chirurgical conservator, fa ă de
1991;126(4):518-22; discussion 523.
cei la care s-a practicat tratament chirurgical radical.
3.
Zaouche A, Haouet K. Traitement chirurgical des
Aici chisturile au avut localizare în segmentele marginale
kystes hydatiques du foie. EMC, Techniques
ale catului, acest lucru permi ând tehnica propriu-zisă
chirurgicales, Appareil digestif. Elsevier Masson
;40-
şi evitând riscul interceptării unor pediculi vasculo-
775.
biliari majori. În ceea ce priveşte tratamentul chirurgical
4.
Hasan HM, El-Sayed OM. Laparoscopic treatment of
laparoscopic, acesta a fost practicat la pacien ii cu chist
liver hydatid cyst. J Med Biomed Sci 2010;1:47-51.
hidatic necomplicat, localizat predominant în
5.
Yagci G, Ustunsoz B, Kaymakcioglu N, et al. Results
segmentele hepatice II-VI marginale.
of surgical, laparoscopic, and percutaneous treatment for
În general, se consideră că interven ia chirurgicală
hydatid disease of the liver: 10 years experience with 355
radicală se înso eşte de un risc intraoperator mai mare,
patients. World J Surg 2005;29(12):1670-9.
cu o rată de recuren ă mai mică, în timp ce abordarea
6.
Belghiti J, Benhamou JP, Houry S, Grenier P, Huguier
chirurgicală conservatoare prezintă un risc perioperator
M, Fékété F. Caustic sclerosing cholangitis. A
mai mic, dar o rată de recuren ă mai mare [12]. Și în
complication of the surgical treatment of hydatid disease
studiul nostru rata morbidită ii și recuren a bolii au fost
of the liver. Arch Surg 1986;121(10):1162-5.
mai mari la pacien ii care au bene ciat de interven ii
7.
Sa oleas M, Misiakos E, Manti C, Katsikas D,
conservatoare, aceștia prezentând un risc crescut pentru
Skalkeas G. Diagnostic evaluation and surgical
stula biliară externă, comparativ cu pacien ii la care s-a
management of hydatid disease of the liver. World J
practicat tratament chirurgical radical. De asemenea
Surg 1994;18(6):859-65.
rata mortalită ii a fost semni cativ mai mare în rândul
8.
Morris DL, Dykes PW, Dickson B, Marriner SE,
pacien ilor trata i chirurgical clasic, comparativ cu cei
Bogan JA, Burrows FG. Albendazole in hydatid disease.
trata i laparoscopic.
Br Med J (Clin Res Ed) 1983;286(6359):103-4.
Mai multe rapoarte au con rmat posibilitatea
9.
Queiroz-Medeiros M, Menezes-Silva A, Raposo-
aplicării chirurgiei laparoscopice în boala hidatică
D’Almeida, et al. Surgical treatment of hepatic hydatid
hepatică [4,13,14], deși controverse în ceea ce privește
disease. European IHPBA Congress, Hamburg 97,
rolul laparoscopiei în gestionarea bolii hidatice nu au fost
Monduzzi editore, International Proceedings
rezolvate până în prezent [4,15]. Studiul de fa ă
Division, Bologna 1997;229-33.
demonstreză că abordul chirurgical laparoscopic este
10.
Gil-Grande LA, Boixeda D, Ledo L. Tratamiento
News in the Treatment of Hepatic Hydatid Cyst
121
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
actual de la hydatidosis humana. Enferm Infect
13. Sağlam A. Laparoscopic treatment of liver hydatid cysts.
Microbiol Clin 1987;5:627-32.
Surg Laparosc Endosc 1996;6(1):16-21.
11. Gil-Grande LA, Rodriguez Caabeiro F, et al. Randomised
14. Ertem M, Karahasanoglu T, Yavuz N, Erguney S.
controlled trial of e cacy of albendazole in intraabdominal
Laparoscopically treated liver hydatid cysts. Arch Surg
hydatid disease. Lancet 1993;342:1269-72.
2002;137(10):1170-3.
12. Filice C, Pirola F, Brunetti E, Dughetti S, Strosselli M,
15. Bickel A, Daud G, Urbach D, Le er E, Barasch EF,
Foglieni CS. A new therapeutic approach for hydatid liver
Eitan A. Laparoscopic approach to hydatid liver cysts. Is
cysts. Aspiration and alcohol injection under sonographic
it logical? Physical, experimental, and practical aspects.
guidance. Gastroenterology. 1990;98(5 Pt 1):1366-8.
Surg Endosc 1998;12(8):1073-7.
122
Nichita et al
ORIGINAL ARTICLES
COMPARAȚIE ÎNTRE METODELE CHIRURGICALE CLASICE ȘI
LAPAROSCOPICE ÎN PATOLOGIA BENIGNĂ TUBO OVARIANĂ
Nicolae Babău1, Marius Sebastian Teodorescu2
1Clinica Chirurgie Generală II, Spitalul Clinic Jude ean de Urgen ă Oradea, Facultatea de Medicină și Farmacie Oradea,
2Clinica Chirurgie I, Spitalul Clinic Jude ean de Urgen ă Timișoara, Universitatea de Medicină și Farmacie „Victor
Babeș” Timișoara, România
Adresa pentru coresponden ă:
Dr. Nicolae Babău
Facultatea de Medicină și Farmacie Oradea
Pia a 1 Decembrie 10, 410073 Oradea, România
Tel: +40758433533/+40770715527
E-mail: nicolae.babau@gmail.com
Primit: 05.08.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 123-133
Rezumat
chirurgicale și patologice, indicii de operare,
morbiditatea și indicii de spitalizare.
Introducere: Patologia regiunii tubo-ovariene este
Rezultate: Analizând indicii de operare, am
foarte complexă, ca atare și managementul terapeutic,
constatat că timpul de operare a fost în medie de 90,81
medicamentos și chirurgical va
deosebit de variat,
minute pentru laparoscopie, comparativ cu laparotomia,
nemaivorbind că trebuie să e individualizat. În ultimii
unde acesta a fost în medie de 81,16 minute (p<0,0001).
ani chirurgia laparoscopică a luat amploare în chirurgia
Pierderea de sânge intraoperator a fost semni cativ mai
sferei genitale. Multe proceduri efectuate anterior ca
scăzută în lotul pacientelor tratate laparoscopic,
opera ii tradi ionale abdominale și vaginale sunt fezabile
comparativ cu cele tratate prin laparotomie (78±41,80
sau chiar ușor de realizat prin laparoscopie.
versus 157±84,59; p<0,0001). Cel mai mic procent de
Scopul acestui studiu este de a evalua fezabilitatea,
satura ie în oxigen a fost de
99%, fără diferen e
siguran a şi e cien a tratamentului laparoscopic versus
semni cative între loturi. Cistita a predominat la
laparotomia conven ională, în patologia benignă a
pacientele tratate laparoscopic, în timp ce infec ia
regiunii tubo-ovariene.
pelvică și infec ia plăgii operatorii au predominat la
Material și metode: Studiul s-a realizat pe un
pacientele tratate prin laparotomie
(p<0,05). Trei
număr de 1238 de cazuri cu patologie benignă în sfera
paciente au necesitat transfuzie de sânge după o sarcină
tubo-ovariană, dintre care 636 de cazuri (520 tumori
ectopică ruptă, una tratată laparoscopic și două tratate
ovariene benigne, 28 torsiuni de anexă, 28 abcese tubo-
prin laparotomie. Doza parenterală postoperatorie de
ovariene și 60 sarcini tubare) au fost tratate chirurgical
analgezic și doza postoperatorie de antiemetic au fost
prin laparoscopie și 602 cazuri (436 tumori ovariene
semni cativ mai scăzute după laparoscopie, comparativ
benigne, 12 torsiuni de anexă, 94 abcese tubo-ovariene
cu laparotomia (p<0,0001). Morbiditatea febrilă a fost
și
60 sarcini tubare) au fost tratate chirurgical prin
găsită la 19 paciente tratate laparoscopic, comparativ cu
laparotomie. Ambele grupuri au fost comparate în
139 paciente tratate prin laparotomie (p<0,000001).
func ie de caracteristicile demogra ce, indica iile
Indicii spitalicești arată o perioadă de spitalizare
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
123
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
postoperatorie și o perioadă de recuperare postoperatorie
intra- și post-operatorii, morbiditatea febrilă, perioada
semni cativ mai mică în lotul pacientelor tratate
de spitalizare postoperatorie și perioada de recuperare
laparoscopic, comparativ cu lotul celor tratate prin
postoperatorie.
laparotomie (p<0,0001).
Concluzii: Studiul de fa ă demonstrează
Material și metode
fezabilitatea, siguran a şi e cien a tratamentului
laparoscopic comparativ cu laparotomia conven ională,
Acest studiu observa ional, retospectiv și de cohortă
în patologia benignă a regiunii tubo-ovariene.
s-a desfășurat în perioada 2000-2012, pe un număr de
Cuvinte cheie: Laparoscopie, laparotomie, patologie
1238 de cazuri cu patologie benignă tubo-ovariană,
benignă tubo-ovariană
internate în sec ia Chirurgie II a Spitalului Clinic
Jude ean de Urgen ă Oradea.
Introducere
Criteriile de includere: vârsta peste 18 ani, tumori
ovariene benigne, sarcină tubară cu semne vitale stabile,
Patologia regiunii tubo-ovariene este complexă, ca
torsiune de anexă, abces tubo-ovarian, anexe libere sau
atare și managemetul terapeutic, medicamentos și
care ar putea mobilizate în condi ii de siguran ă prin
chirurgical, trebuie să e individualizat și să ină cont de
laparoscopie, stabilitate hemodinamică, expunerea
vârstă, starea clinică și dorin ele pacientei, informată în
câmpului operator adecvată (lipsa aderen elor).
mod corespunzător.
Criteriile de excludere: vârsta sub 18 ani și semne de
Datorită importan ei ovarului pentru echilibrul
malignitate tubară sau ovariană. Indica iile chirurgicale
hormonal şi func ia de reproducere la femeia tânără,
au fost tumori ovariene benigne, torsiune de anexă,
este evident că tehnicile chirurgicale conservatoare au
abces tubo-ovarian sau sarcina tubară cu semne vitale
prioritate ori de câte ori este posibil.
stabile.
În ultimii ani laparoscopia chirurgicală a luat
Toate pacientele au avut un indice de masă corporală
amploare în chirurgia sferei genitale. Multe proceduri
<30 kg/m2. În cazurile de tumori ovariene, s-a făcut o
efectuate anterior ca opera ii tradi ionale abdominale și
selec ie atentă pe baza istoricului bolii, vârstei pacientei,
vaginale sunt fezabile sau chiar ușor de realizat prin
constatărilor clinice și ecogra ei precum și determinării
laparoscopie. Tehnica de bază este bine descrisă în
serice a markerului CA-125. Deoarece pentru pacientele
detaliu în literatură [1]. Multiplele avantaje ale metodei
a ate în premenopauză speci citatea testului este
sunt: scăderea pierderii de sânge intraoperator, scăderea
redusă, în cazul unei suspiciuni de malignitate
formării de aderen e, reducerea perioadei de spitalizare,
intraoperatorie s-a prelevat esut pentru examenul
a durerii postoperatorii și a perioadei de recuperare
microscopic extemporaneu. Rezultatul pozitiv a impus
postoperatorie. Pe lângă acestea, în compara ie cu
continuarea opera iei prin laparotomie de stadializare
laparotomia, are și dezavantaje care-i limiteză
chirurgicală. În cazul în care malignitatea a fost
poten ialul: expunerea câmpului operator poate
diagnosticată după chirurgia laparoscopică, tratamentul
redusă, instrumentele sunt mici și pot folosite numai
chirurgical pentru cancer s-a realizat în termen de o
prin porturi xe, capacitatea de a manipula viscerele
săptămână. După inducerea anesteziei generale, s-a
pelviene este limitată. În unele cazuri, costul de
efectuat o examinare laparoscopică a pelvisului și
spitalizare crește, în ciuda perioadei scurte de spitalizare,
abdomenului superior în scop diagnostic. Chirurgia
din cauza timpului prelungit în sala de opera ie și
laparoscopică de ovar a fost efectuată atunci când au fost
utilizării de echipamente chirurgicale și consumabile
îndeplinite criteriile de includere.
mai scumpe. Este nevoie de abilitate, pregătire și
Lotul de cercetare a cuprins 636 de paciente, din
experien ă adecvate pentru a reduce complica iile.
care
520 sufereau de tumori ovariene benigne,
28
Timpul operator este comparabil cu cel al laparotomiei
torsiuni de anexă, 28 abcese tubo-ovariene și 60 sarcini
[2,3].
tubare. Lotul control a fost alcătuit din cazuri tratate în
Scopul acestui studiu este de a evalua fezabilitatea,
aceeași perioadă, având grad de di cultate chirurgicală
siguran a şi e cien a tratamentului laparoscopic versus
cu indica ie pentru laparotomie. Acestea au fost evaluate
laparotomia conven ională, în patologia benignă a
retrospectiv pentru compara ie: 602 de cazuri, dintre
regiunii tubo-ovariene, urmărind ca și parametrii post-
care 436 tumori ovariene benigne, 12 torsiuni de anexă,
operatori: timpul de operare, doza postoperatorie de
94 abcese tubo-ovariene și 60 sarcini tubare.
antiemetic, doza parenterală postoperatorie de analgezic,
Recuperarea postoperatorie a fost de nită ca timpul
pierderea de sânge, cel mai mic procent de satura ie în
(evaluat în zile) necesar pacientei pentru să-și relua
oxigen în timpul interven iei chirurgicale, complica iile
activită ile zilnice și/sau de lucru normale. Pro laxia cu
124
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
antibiotice nu a fost utilizată în mod obișnuit în ecare
Tabelul I. Distribu ia cazurilor de patologie tubo-
ovariană benignă în func ie de localizarea anatomică
grup, cu excep ia abcesului tubo-ovarian.
Complica iile au fost de nite ca ind acele evenimente
Patologie tubo-ovariană benignă (n=1238)
care au necesitat tratament activ, sau o spitalizare prelungită.
Trompa uterină
Morbiditatea febrilă a fost de nită ca temperatură >38°C,
Sarcina ectopică
120 (9,69%)
p†
măsurată de două ori la interval de 24 de ore postoperator,
Ovar
956 (77,22%)
cu excep ia primelor 24 de ore postoperator. După vizita
Chist func ional
129 (13,49%)
de reevaluare clinică la 4 săptămâni postoperator, pacientele
Chist endometrionic
292 (30,54%)
au revenit la activitatea normală.
Chist dermoid
267 (27,93%)
Variabilele evaluate au fost: vârsta, paritatea,
Chist mucinos
84 (8,79%)
premenopauza, menopauza, indicele de masă corporală,
Chist seros
97 (10,15%)
p<0,0001*
diametrul chistului ovarian, diametrul abcesului tubo-
Chist parovarian
22 (2,30%)
ovarian, utilizarea și durata utilizării dispozitivului
Fibrom
28 (2,93%)
intrauterin (DIU), indica iile chirurgicale și patologice,
Altele (hidrosalpinx/chist
37 (3,87%)
timpul de operare, doza postoperatorie de antiemetic,
simplu)
doza parenterală postoperatorie de analgezic, pierderea de
Trompă și ovar
sânge, cel mai mic procent de satura ie în oxigen în timpul
Abces tubo-ovarian
122 (9,85%)
interven iei chirurgicale, complica iile intra- și post-
Torsiune de anexă
40 (3,23%)
operatorii, morbiditatea febrilă, perioada de spitalizare
p†
p<0,0001*
postoperatorie și perioada de recuperare postoperatorie.
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile
studiate
Datele au fost colectate retrospectiv din foile de
* Chi-square test
observa ie, stocate şi prelucrate cu ajutorul programului
** Fisher’s exact test
Microsoft® Excel®
2010
(Microsoft® Corporation,
SUA), constituind baza de date a studiului statistic.
Ca metode de analiză statistică au fost folosite testul
de chistul dermoid, func ional, seros, mucinos cu
Chi-pătrat, Fisher’s exact test, Comparison of means
diferen ă semni cativă statistic (p<0,0001). Un procent
test, Comparison of proportions test, Relative risk test şi
mic de paciente au avut hidrosalpinx, chist simplu,
calcularea coe cientului de corela ie utilizând programul
brom ovarian și chist parovarian.
de statistică medicală MedCalc® versiunea
12.2.1.0
Cele
1.238 cazuri de patologie tubo-ovariană
benignă au fost împăr ite în două loturi:
(MedCalc® Software, Mariakerke, Belgium).
Studiul a fost aprobat de comisia de avizare internă
Lotul de studiu (Lotul S) - format din 636 de
a lucrărilor de cercetare-dezvoltare din cadrul spitalului
paciente (520 tumori ovariene benigne, 28 torsiuni de
și toate pacientele au fost rugate să completeze și să
anexă, 28 abcese tubo-ovariene și 60 sarcini tubare)
semneze un formular de consim ământ informat, după
tratate chirurgical prin laparoscopie.
ce li s-au explicat riscurile și complica iile, inclusiv
Lotul control (Lotul C) - format din 602 de cazuri
șansele de conversie a laparoscopiei la laparotomie.
cu patologie tubo-ovariană benignă
(436 tumori
ovariene benigne, 12 torsiuni de anexă, 94 abcese tubo-
Rezultate
ovariene și
60 sarcini tubare), potrivite ca indica ie,
procedură și grad de di cultate chirurgicală pentru
S-au luat în studiu 1.238 de cazuri cu patologie
laparotomie.
benignă în sfera tubo-ovariană, internate în sec ia
Ambele grupuri au fost comparate în func ie de
Chirurgie II a Spitalului Clinic Jude ean de Urgen ă
caracteristicile demogra ce, indica iile chirurgicale și
Oradea. Patologia tubo-ovariană benignă a fost
patologie (Tabelul II).
caracterizată prin prezen a patologiei benigne tubare
Vârsta, ca și factor epidemiologic, are o mare
(sarcină ectopică), ovariene (tumori ovariene benigne),
importan ă în patologia tubo-ovariană, unele afec iuni
sau tubo-ovariene
(torsiune de anexă, abces tubo-
din această sferă sunt net predilecte la anumite vârste,
ovarian)
(Tabelul I). Analizând rezultatele statistice,
ind in uen ate de modi cările hormonale, dar şi de
putem observa că majoritatea pacientelor internate au
obiceiurile sexuale. În studiul nostru madia de vârstă a
avut tumori ovariene benigne
(77,22%), urmate de
pacientelor cu patologie tubo-ovariană a fost în jur de
abcesul tubo-ovarian, sarcina ectopică și torsiunea de
34-35 ani, cu un interval de vârstă între 17-58 ani, fără
anexă
(p<0,0001). Între tumorile benigne ovariene,
diferen e semni cative statistic între cele două loturi
chistul edometrionic a fost majoritar (30,54%), urmat
studiate (Tabelul II). Indicele de masă corporală a fost
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
125
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Tabelul II. Caracteristici demogra ce, clinice și paraclinice
Lotul S
Lotul C
Date
p†
n=636
n=602
Vârstă (ani)
(17-56) 34,8±8,3
(20-58) 34,5±5,8
p=0,4544*
urban
312
289
p=1,000000**
Mediul de provenien ă
rural
324
313
p=1,000000**
Paritate
(1-3) 2,1±1,2
(1-3) 2,0±1,1
p=0,1211*
Perioada fertilă
584
572
p=0,029359**
Menopauză
52
30
p=0,029359**
Indexul masei corporale (kg/m2)
21,2±2,6
21,4±2,5
p=0,1617*
Diametrul ecogra c al chistului ovarian (cm) (media)
(4-5) 4,48±0,5
(4-12) 7,98±2,53
p<0,0001*
Diametrul ecogra c al abcesului (cm) (media)
(4-7) 5,58±1,09
(7-10) 8,54±1,12
p<0,0001*
p<0,0001****
Utilizarea DIU*
9
58
RR=1,0910
Durata utilizării DIU (ani)
(2-5) 3,52±1,13
(5-10) 7,40±1,70
p<0,0001*
Indica ii chirurgicale
Masă pelvină
137 (21,5%)
149 (24,75%)
p=1,000000**
Dismenoree
117 (18,4%)
142 (23,59%)
p=1,000000**
Durere acută pelvină
574 (90,3%)
543 (90,20%)
p=1,000000**
Durere cronică pelvină
62 (9,7%)
59 (9,80%)
p=1,000000**
Tulburări menstruale
78 (12,2%)
88 (14,62%)
p=1,000000**
Aderen e pelvine (ușoare-moderate)
69 (10,8%)
38 (6,31%)
p=0,004591**
p†
p<0,0001***
p<0,0001***
Patologie benignă
Ovariană
520
436
p=1,000000**
chist func ional
85 (16,3%)
44 (10,2%)
p=1,000000**
chist endometrionic
136 (26,2%)
156 (35,8%)
p=1,000000**
chist dermoid
104 (20%)
163 (37,3%)
p=1,000000**
chist mucinos
67 (12,8%)
17 (3,9%)
p=0,000001**
chist seros
67 (12,8%)
30 (6,9%)
p=0,002479**
chist paraovarian
22 (4,2%)
0 (0%)
p=0,000002**
brom
16 (3,1%)
12 (2,8%)
p=0,848527**
Altele (hidrosalpinx/chist simplu)
23 (4,6%)
14 (3,1%)
p=0,400941**
p†
p<0,0001***
p<0,0001***
Trompă uterină
Sarcină ectopică
60 (9,44%)
60 (9,39%)
p=1,000000**
Torsiune de anexă
28 (4,4%)
12 (1,87%)
p=0,010123**
Abces tubo-ovarian
28 (4,4%)
94 (14,72%)
p=1,000000**
p†
p<0,0001***
p<0,0001***
†p<0,05 dovedeşte o diferen ă statistic semni
cativă între loturile studiate
* Comparison of means (t-test)
** Fisher’s exact test
*** Chi-square test
**** Relative risk
<30 kg/m2 la toate pacientele. Provenien a bolnavelor
perioada fertilă și 52 la menopauză, iar în Lotul C, 572
din mediul urban sau rural nu reprezintă un indicator
în perioada fertilă și 30 la menopauză.
care să permită re inerea unor concluzii. Reparti ia
Toate pacientele au fost investigate paraclinic prin
cazurilor nu atestă o diferen ă statistic semni cativă
ecogra e transabdominală, transvaginală și Doppler
între loturi (Tabelul II).
color. Astfel, în cazul în care pacienta a fost diagnosticată
Distribu ia pacientelor cu patologie tubo-ovariană
cu chist ovarian s-a luat în calcul dimensiunea acestuia
în func ie de statusul hormonal a fost în Lotul S, 584 în în privin a unei conduite terapeutice ulterioare. Similar
126
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
s-a procedat și în cazul abcesului tubo-ovarian și sarcinii
ectopice. Indica iile pentru laparoscopie au fost
stabilitatea hemodinamică, diametrul forma iunii
tumorale benigne <10 cm și dorin a păstrării fertilită ii.
Prin urmare, pacientele care au urmat tratament
laparoscopic au avut diametrul chistului ovarian,
respectiv al abcesului tubo-ovarian net mai mic, fa ă de
pacientele tratate prin laparotomie, cu diferen ă
semni cativă între loturi (Tabelul II).
Ca și factor etiologic, utilizarea unui DIU crește
riscul pentru boală in amatorie pelviană
(BIP) și
implicit abces tubo-ovarian. În studiul de fa ă,
9
paciente tratate laparoscopic pentru abces tubo-ovarian
au fost purtătoare de DIU între 2 și 5 ani și 58 de
paciente tratate prin laparotomie pentru abces tubo-
ovarian au fost purtătoare de DIU între 5 și 10 ani, cu
Figura 1. Distribu ia pacientelor pe cele două loturi
în func ie de patologia tubo-ovariană benignă
diferen ă semni cativă statistic între loturi (p<0,05).
Patologia regiunii tubo-ovariene este complexă,
prin urmare şi tabloul clinic este deosebit de variat.
Durerea acută pelvină a fost simptomul principal care a
dominat tabloul clinic în ambele loturi, urmată de
prezen a unei mase pelvine, dismenoreea, tulburările
menstruale, prezen a aderen elor pelvine ușoare
-
moderate la examenul diagnostic laparoscopic și durerea
cronică pelvină, cu diferen ă semni cativă statistic între
variabile (p<0,0001), dar fără importan ă semni cativă
statistic între loturi. Prezen a unei mase pelvine peste
6-10 cm diametru, a aderen elor anexiale severe din
punct de vedere laparoscopic și instabilită ii
hemodinamice, au fost sugestive pentru o boală severă
Figura 2. Distribu ia pacientelor abces tubo-ovarian
cu indica ie chirurgicală prin laparotomie (Tabelul II).
în func ie de procedura cirurgicală
Indica iile pentru chirurgia laparoscopică au fost
tumori ovariene benigne, sarcina tubară, torsiunea de
anexă și abcesul tubo-ovarian cu semne vitale stabile.
salpingo-ovarectomii,
salpingectomii,
ovarectomii
Din punct de vedere statistic nu au existat diferen e
unilaterale, anexectomii unilaterale, histerectomii cu
semni cative între loturi privind patologia tobo-
salpingo-ovarectomii și salpingotomii, cu diferen ă
ovariană, cu excep ia chistului mucinos, seros, parovarian
semni cativă statistic (p<0,0001) (Tabelul III).
și a torsiunii de anexă, care au predominat în lotul
Comparând cele două loturi, putem observa că
pacientelor tratate laparoscopic (Tabelul II; Figura 1).
există diferen e semni cative statistic în cazul
Chisturile ectodermoide, dermatoide și func ionale
ovarectomiei unilaterale, salpingectomiei, care au
au reprezentat mai mult de jumătate (71,93%) din
predominat în lotul pacientelor tratate prin laparotomie.
patologia tumorilor benigne ovariene, umate de
Salpingotomia s-a paracticat doar în cazul pacientelor
chisturile seroase, mucinoase, hidropiosalpinxuri,
tratate laparoscopic, unde sarcina tubară a fost mai mică
chisturi simple, broame ovariene și chisturi parovariene
de 5 cm, sacul gesta ional a fost localizat în ampulă sau
(Tabelul II).
por iunea istmică, s-a dorit păstrarea func iei fertile și
În ceea ce privește tipul interven iei chirurgicale, au
statusul hemodinamic a fost stabil (Tabelul III).
predominat interven iile chirurgicale conservatoare,
Histerectomia cu salpingo-ovarectomie a fost o
având în vedere vârsta fertilă a cazuisticii. Interven iile
interven ie chirurgicală pur laparotomică, practicată în
chirurgicale radicale s-au realizat acolo unde tabloul
cazul pacientelor cu abces tubo-ovarian sever, adică un
clinic și intraoperator a indicat acest lucru.
diametru ecogra c mai mare de 10 cm, cu semne de
Astfel, în lotul total de paciente au predominat
irita ie peritoneală, stare septică și status hemodinamic
chistectomiile în propor ie de
34,08%, urmate de
instabil (Tabelul III; Figura 2).
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
127
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Figura 3. Distribu ia pacientelor cu tumori benigne ovariane
Figura 4. Distribu ia pacientelor cu sarcină ectopică tubară
în func ie de procedura cirurgicală
în func ie de procedura cirurgicală
Tabelul III. Tipul interven iei chirurgicale în func ie de patologia tubo-ovariană
Group S
Group C
p†
n=636
n=602
Tumori ovariene benigne
520
436
Chistectomii
230
166
p=1,000000*
Ovarectomie unilaterală
35
72
p=0,000003*
Salpingo-ovarectomie
232
184
p=1,000000*
Salpingectomie
23
14
p=0,400941*
Sarcină ectopică
60
60
Salpingectomie
12
60
p<0,000001*
Salpingotomie
48
0
p<0,000001*
Torsiune de anexă
28
12
Detorsiune+chistectomie
24
2
p=0,000060*
Anexectomie unilaterală
4
10
p=0,000060*
Abces tubo-ovarian
28
94
Anexectomie unilaterală
28
26
p<0,000001*
Histerectomie cu salpingo-ovarectomie
0
68
p<0,000001*
Total
636
602
Chistectomii
254
168
p=1,000000*
Ovarectomie unilaterală
35
72
p=0,000068*
Salpingo-ovarectomie
232
184
p=1,000000*
Salpingectomie
35
74
p=0,000032*
Salpingotomie
48
0
p<0,000001*
Anexectomie unilaterală
32
36
p=0,532985*
Histerectomie cu salpingo-ovarectomie
0
68
p<0,000001*
p†
p<0,0001** p<0,0001**
†p<0,05 dovedeşte o diferen ă statistic semni
cativă între loturile studiate
* Fisher’s exact test
** Chi-square test
Analizând frecven a interven iilor chirurgicale pe
Diferen e semni cative statistic între
cele
două
patologii, putem observa că în cazul tumorilor ovariene
loturi s-au înregistrat și în cazul sarcinii ectopice, unde
benigne, mai numeroase au fost chistectomiile, urmate
salpingectomia a predominat la pacientele tratate prin
de salpingo-ovarectomii, ovarectomii unilaterale și
laparotomie (60 vs. 12). Această indica ie chirurgicală a
salpingectomii, fără diferen e semni cative statistic, cu
fost determinată de prezen a tabloului clinic sever
excep ia ovarectomiei unilaterale, care s-a practicat la un
caracterizat prin prezen a instabilită ii hemodinamice,
număr mai mare de cazuri din lotul pacientelor tratate
hemoperitoneului și mărimea sacului gesta ional peste 5
prin laparotomie (Tabelul III; Figura 3).
cm, care a dus în multe cazuri la ruptura trompei
128
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
Figura 5. Distribu ia pacientelor cu torsiune de anexă
Figura 6. Distribu ia pacientelor cu patologie tubo-ovariană
în func ie de procedura cirurgicală
benignă în func ie de media indicilor de operare
și postoperare
Tabelul IV. Rezultatele privind indicii de operare, morbiditatea și indicii de spitalizare între cele două loturi
Lotul S
Lotul C
p†
n=636
n=602
Timpul de operare (min.)
90,81±18,12 (60-120)
81,16±23,46 (40-120)
p<0,0001*
Doza postoperatorie de antiemetic (mg)
3,8±4,7
5,9±9,1
p<0,0001**
Doza parenterală postoperatorie de analgezic (mg)
10,5±21,8
149,8±81
p<0,0001**
pierderea de sânge (ml)
78±41,80 (5-150)
157±84,59 (20-600)
p<0,0001*
Cel mai mic procent de satura ie în oxigen (%)
99,1±0,7
99,1±0,4
p=1,0000**
Complica ii post-operatorii
37 (5,81%)
48 (7,97%)
p=0,144552***
Cistită
28 (4,4%)
12 (1,99%)
p=0,023237***
Infec ie pelvică
0
12 (1,99%)
Infec ia plăgii chirurgicale
8 (1,25%)
22 (3,65%)
p=0,020260***
Transfuzie de sânge
1 (0,15%)
2 (0,33%)
p=1,000000***
Morbiditatea febrilă
19 (3,1%)
139 (23,1%)
p<0,000001***
Perioada de spitalizare postoperatorie (zile)
3,0±1,0
5,0±1,3
p<0,0001**
Perioada de recuperare postoperatorie (săptămâni)
1,0±0,3
3,0±0,3
p<0,0001**
†p<0,05 dovedeşte o diferen ă statistic semni cativă între loturile studiate
* testul Mann-Whitney
** Comparison of means (t-test)
*** Fisher’s exact test
uterine. În lotul pacientelor tratate laparoscopic,
laparoscopie, comparativ cu laparotomia, unde acesta a
salpingectomia s-a realizat în condi ii de stabilitate
fost în medie de 81,16 minute (p<0,0001). Pierderea de
hemodinamică (Tabelul III; Figura 4).
sânge intraoperator a fost semni cativ mai scăzută în
85,71% din pacientele tratate laparoscopic pentru
lotul pacientelor tratate laparoscopic, comparativ cu cele
torsiune de anexă, inându-se cont de păstrarea func iei
tratate prin laparotomie (78±41,80 versus 157±84,59;
ovariene și implicit a func iei fertile, având în vedere
p<0,0001) (Tabelul IV; Figura 6). Cel mai mic procent
pacientura tânără, s-a practicat detorsiunea chirurgicală,
de satura ie în oxigen a fost de 99%, fără diferen e
asociată cu chistectomie. Anexectomia unilaterală a fost
semni cative între loturi.
rezervată pacientelor a ate la menopauză și în cazul în
Complica iile postoperatorii au fost mai frecvente în
care uxul sanguin și culoarea normală a ovarului nu au
grupul cu laparotomie, comparativ cu lotul de studiu.
putut
restabilite după detorsiunea chirurgicală.
Acestea au reprezentat cistite, infec ii pelvice, infec ii ale
Aceasta s-a practicat predominant la pacientele tratate
plăgii operatorii și transfuzii de sânge. Diferen e
prin laparotomie, cu diferen ă semni cativă statistic
semni cative statistic între cele două loturi au fost în
între cele două loturi (Tabelul III; Figura 5).
cazul cistitei, care a predominat la pacientele tratate
Analizând indicii de operare, am constatat că timpul
laparoscopic, infec iei pelvice și infec iei plăgii operatorii,
de operare a fost în medie de 90,81 minute pentru care au predominat la pacientele tratate prin laparotomie
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
129
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
1000 de femei, cu o inciden ă de vârf de aproximativ 20
de cazuri la 1000 de femei cu vârsta cuprinsă între 20-
24 de ani [5].
Un fapt real con rmat prin studii statistice, este că
75% din BIP sunt cauzate de boli cu transmitere sexuală,
20% de manevre iatrogene, iar avortul şi infec iile
puerperale au o inciden ă ce se apropie de 5%. Conform
estimărilor OMS 2008, 499 de milioane de noi cazuri
de infec ii cu transmitere sexuală curabile (de exemplu
si lis, gonoree, chlamydia, tricomoniază) au loc anual în
întreaga lume, la adul ii cu vârsta cuprinsă între 15-49
de ani [6]. BIP este cel mai frecvent observată la femeile
Figura 7. Distribu ia pacientelor cu patologie tubo-ovariană
benignă în func ie de perioada de spitalizare/recuperare
tinere și foarte rar la femeile în postmenopauză. Mai
pu in de 2% din femeile a ate la menopauză au BIP [7].
Prin urmare factorii de risc pentru BIP includ mai mul i
(p<0,05). Trei paciente au necesitat transfuzie de sânge
parteneri sexuali, o istorie de boli cu transmitere sexuală
după o sarcină ectopică ruptă, una tratată laparoscopic și
anterioră și un istoric de abuz sexual
[8]. Proceduri
două tratate prin laparotomie, această complica ie ind
chirurgicale ginecologice, cum ar
biopsia de
fără semni ca ie statistică (Tabelul IV).
endometru, chiuretajul și histeroscopia ce penetrează
De asemenea, doza parenterală postoperatorie de
bariera colului uterin, predispun femeile la infec ii
analgezic și doza postoperatorie de antiemetic au fost
ascendente [9,10].
semni cativ mai scăzute după laparoscopie, comparativ
De asemenea, orice femeie cu ovare func ionale
cu laparotomia (p<0,0001) (Tabelul IV).
poate avea o sarcină extrauterină, începând cu vârsta
Morbiditatea febrilă de nită ca temperatură >38°C,
menarhei până la menopauză. Femeile în vârstă de 40 de
măsurată de două ori la interval de 24 de ore postoperator,
ani s-au dovedit a avea un raport de cote ajustat de 2,9
cu excep ia primelor 24 de ore postoperator, a fost găsită
pentru sarcină extrauterină [11]. Cea mai mare rată a
la 19 paciente tratate laparoscopic, comparativ cu 139
sarcinii ectopice apare la femei cu vârsta cuprinsă între
paciente tratate prin laparotomie (p<0,000001) (Tabelul
35-44 de ani. O explica ie sugerează că îmbătrânirea
IV).
poate duce la o pierdere progresivă a activită ii
Pro laxia cu antibiotice nu a fost utilizată în mod
mioelectrice în trompa uterină, responsabilă pentru
obișnuit, în ecare grup, cu excep ia abcesului tubo-
motilitatea trompelor uterine [12].
ovarian.
Chisturile ovariene, de departe cea mai frecventă
Indicii spitalicești arată o perioadă de spitalizare
afec iune după cum se vede şi din statistica noastră
postoperatorie și o perioadă de recuperare postoperatorie
(71,97%) fără a detalia clasi carea lor, sunt apanajul
semni cativ mai mică în lotul pacientelor tratate
perioadei „menstruale” a femeii, având în vedere că în
laparoscopic, comparativ cu lotul celor tratate prin
mecanismul de producere schimbările hormonale au
laparotomie (p<0,0001) (Tabelul IV; Figura 7). După
rol determinant. Se observă din studiul efectuat, o
vizita de reevaluare clinică la 4 săptămâni postoperator,
predominan ă clară a acestei patologii în perioadele
pacientele au revenit la activitatea normală.
extreme ale vie ii genitale, pubertate şi premenopauză,
când şi tulburările de corela ie hipotalamo-hipo zo-
Discuții
ovariene sunt mai frecvente. Chisturile ovariene
func ionale pot apărea la orice vârstă
(inclusiv in
Vârsta, considerată factor epidemiologic, are o mare
utero), dar sunt mult mai frecvente la femeile de vârstă
importan ă în patologia tubo-ovariană, unele afec iuni
reproductivă. Ele sunt rare după menopauză.
din această sferă sunt net predilecte la anumite vârste,
Chisturile luteale apar după ovula ie la femei de vârsta
ind in uen ate de modi cările hormonale, dar şi de
reproductivă. Majoritatea chisturilor benigne apar în
obiceiurile sexuale.
timpul anilor de fertilitate, dar intervalul de vârstă
Anual, aproximativ 1 milion de femei dezvoltă BIP
este larg și ele pot să apară la persoane de orice vârstă
[4]. Se estimează că aproximativ una din opt adolescente
[13].
active sexual dezvoltă BIP înainte de împlinirea vârstei
Raportat la datele epidemiologice din literatură și în
de 20 ani. Inciden a anuală a BIP la femeile cu vârsta
studiul nostru madia de vârstă a pacientelor cu patologie
cuprinsă între 15-39 de ani pare a de 10-13 cazuri la
tubo-ovariană a fost în jur de 34-35 ani, cu un interval
130
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
de vârstă între 18-58 ani, fără diferen e semni cative
chisturi corpus luteum și tumori dermoide [19]. Și în
statistic între cele două loturi studiate.
studiul nostru rezultatele distribu iei tumorilor ovariene
Provenien a bolnavelor din mediul urban sau rural
benigne corespund cu cele din literatură, având
nu reprezintă un indicator care să permită concluzii.
semni ca ie statistică
(p<0,0001). Astfel, chisturile
Reparti ia cazurilor nu atestă o diferen ă statistic
ectodermoide, dermatoide și func ionale au reprezentat
semni cativă între loturi.
mai mult de jumătate (71,93%) din patologia tumorilor
Similar cu literatura, studiul de fa ă demonstrează
benigne ovariene, urmate de chisturile seroase,
că femeile a ate la vârsta fertilă, cu o via ă activă din
mucinoase, hidropiosalpinxuri, chisturi simple,
punct de vedere sexual, sunt mai expuse riscului de boli
broame ovariene și chisturi parovariene.
din sfera patologiei tubo-ovariene benigne, fa ă de cele
Statistic nu au existat diferen e semni cative între
la care menopauza s-a instalat. Paritatea nu a înregistrat
loturi privind patologia tobo-ovariană, cu excep ia
diferen e semni cative statistic între loturi.
chistului mucinos, seros, parovarian și a torsiunii de
Utilizarea unui DIU a fost legată de un risc de 2
anexă, care au predominat în lotul pacientelor tratate
până la 9 ori mai mare pentru BIP și implicit abcesul
laparoscopic.
tubo-ovarian, dar DIU folosite curent pot reprezenta un
Având în vedere vârsta fertilă a cazuisticii,
risc substan ial mai mic [14]. Într-un studiu retrospectiv
interven iile chirurgicale au fost conservatoare.
de cohortă mare din 2012, riscul global de BIP la
Indica iile pentru laparoscopie au fost stabilitatea
femeile care au avut DIU a fost de 0,54% [15]. Kelly și
hemodinamică, diametrul forma iunii tumorale benigne
colab. au raportat 9,6 cazuri de BIP la 1000 inser ii
<10 cm și dorin a păstrării fertilită ii. Laparotomia a
DIU, cu riscul cel mai semni cativ în primele 20 de zile
fost indicată în cazurile cu instabilitate hemodinamică.
[16]. Meirik și colab. au validat riscul pentru BIP în
În lotul total de paciente au predominat
prima lună după inserare, acesta ind legat de numărul
chistectomiile în propor ie de
34,08%, urmate de
de parteneri sexuali, vârsta pacientei și prevalen a bolilor
salpingo-ovarectomii,
salpingectomii,
ovarectomii
cu transmitere sexuală
[17]. Și în studiul nostru
unilaterale, anexectomii unilaterale, histerectomii cu
pacientele purtătoare de DIU au avut un risc crescut de
salpingo-ovarectomii și salpingostomii, cu diferen ă
apari ie a abcesului tubo-ovarian, cu diferen ă
semni cativă statistic.
semni cativă statistic între loturi (p<0,05).
Comparând cele două loturi, putem observa că
Patologia regiunii tubo-ovariene s-a dovedit a
există diferen e semni cative statistic în cazul
complexă, prin urmare şi tabloul clinic este deosebit de
ovarectomiei unilaterale, salpingectomiei, care au
variat. Dacă durerea acută pelvină și prezen a unei mase
predominat în lotul pacientelor tratate prin laparotomie.
pelvine sunt simptome și semne caracteristice pentru o
Salpingotomia s-a paracticat doar în cazul
patologie acută pelvină, cum ar un chist ovarian mai
pacientelor tratate laparoscopic, unde sarcina tubară a
voluminos, un abces tubo-ovarian, o sarcină ectopică
fost mai mică de 5 cm, sacul gesta ional a fost localizat
sau torsiune de anexă, cu siguran ă dismenoreea,
în ampulă sau por iunea istmică, s-a dorit păstrarea
tulburările menstruale, prezen a aderen elor pelvine și
func iei fertile și statusul hemodinamic a fost stabil.
durerea cronică pelvină au fost sugestive pentru boala
Histerctomia cu salpingo-ovarectomie a fost o
in amatorie pelvină, incluzând endometrioza pelvină și
interven ie chirurgicală pur laparotomică, practicată în
tot ce implică această boală. Durerea acută pelvină a fost
cazul pacientelor cu abces tubo-ovarian sever, adică un
simptomul principal care a dominat tabloul clinic în
diametru ecogra c mai mare de 10 cm, cu semne de
ambele loturi, urmată de prezen a unei mase pelvine,
irita ie peritoneală, stare septică și status hemodinamic
dismenoreea,
tulburările
menstruale,
prezen a
instabil.
aderen elor pelvine ușoare-moderate la examenul
Rota ia anexelor în jurul pediculului vascular poate
diagnostic laparoscopic și durerea cronică pelvină, cu
duce la ocluzia totală sau par ială a alimentării cu sânge,
diferen ă semni cativă statistic între variabile.
ducând la semne zice și simptome compatibile cu un
Lok și colab. [18], într-un studiu realizat pe 500 de
abdomen acut, care poate progresa poten ial într-o
femei operate laparoscopic pentru patologie chistică
urgen ă chirurgicală. Acest lucru are legătură comună cu
ovariană, au constatat endometrioamele
(44,5%) și
prezen a chisturilor
[20]. Evaluarea și tratamentul
chistele dermoide (24,3%) care au reprezentat mai mult
chirurgical laparoscopic este indicat pentru a preveni
de două treimi din cazuri, urmate de chisturile
deteriorarea în continuare a ovarului. Descargues și
func ionale (6,6%). Distribu ia patologică într-un alt
colab. au evaluat 41 de cazuri de torsiune ovariană la
studiu mare a inclus, în ordinea frecven ei,
femeile care s-au prezentat cu durere, grea ă, vărsături și
endometrioame, adenoame benigne, chisturi foliculare,
leucocitoză [21]. Treisprezece paciente au fost tratate
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
131
ORIGINAL ARTICLES
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
laparoscopic, dintre care
11 au fost supuse unui
acestă complica ie ind fără semni ca ie statistică. Doza
tratament conservator, cu detorsionea anexei, iar două
parenterală postoperatorie de analgezic și doza
ovarectomiei. Niciuna dintre aceste paciente nu au avut
postoperatorie de antiemetic au fost semni cativ mai
complica ii chirurgicale. Shalev și Peleg au tratat 41 de
scăzute după laparoscopie, comparativ cu laparotomia;
paciente cu torsiune de anexă prin detorsiune
morbiditatea febrilă de nită ca temperatură
>38°C,
laparoscopică, raportând o recuperare postoperatorie
măsurată de două ori la interval de 24 de ore postoperator,
lipsită de evenimente, cu restabilirea func iei ovariene la
cu excep ia primelor 24 de ore postoperator, a fost găsită
14 paciente [22]. Cohen și colab. au evaluat 58 de cazuri
la 19 paciente tratate laparoscopic, comparativ cu 139
de torsiune ovariană cu ischemie anexială întâlnită la
paciente tratate prin laparotomie. Perioada de spitalizare
laparoscopie și gestionate conservator prin detorsiune
postoperatorie și perioada de recuperare postoperatorie
[23]. Oelsner și colab. au analizat un total de 102 de
au fost semni cativ mai mici în lotul pacientelor tratate
paciente,
67 tratate prin laparoscopie și
35 prin
laparoscopic, comparativ cu lotul celor tratate prin
laparotomie, pentru a determina dacă ovarul își reia
laparotomie.
func ia normală după detorsiunea simplă [24]. 93%
În concluzie, studiul de fa ă demonstrează
dintre pacientele tratate prin laparoscopie au avut
fezabilitatea, siguran a şi e cien a tratamentului
recuperarea completă a func iei foliculare evaluată prin
laparoscopic comparativ cu laparotomia conven ională,
ecogra e
transvaginală,
observând
complica ii
în patologia benignă a regiunii tubo-ovariene.
semni cativ mai pu ine intraoperatorii în grupul
laparoscopic comparativ cu grupul tratat prin
laparotomie. Oelsner și colab. de asemenea, au raportat
Referințe
într-un studiu separat, că 88-100% dintre paciente își
recuperează func ia ovariană, indiferent de aspectul
1.
Medeiros LR, Stein AT, Fachel J, Garry R, Furness S.
ini ial al ovarului afectat [25]. Studiul nostru abordează
Laparoscopy versus laparotomy for benign ovarian
și el acestă atitudine terapeutică într-un procent de
tumor: a systematic review and meta-analysis. Int J
85,71% la pacientele tratate laparoscopic, inându-se
Gynecol Cancer 2008;18(3):387-99.
cont de păstrarea func iei ovariene și implicit a func iei
2.
Nezhat CR, Nezhat FR, Metzger DA, Luciano AA.
fertile, având în vedere pacientura tânără. Anexectomia
Adhesion reformation after reproductive surgery by
unilaterală a fost rezervată pacientelor a ate la
videolaseroscopy. Fertil Steri 1990; 53(6):1008-11.
menopauză și în cazul în care uxul sanguin și culoarea
3.
Berek & Novak’s. Gynecology - 15th ed.,2012 by
normală a ovarului nu au putut
restabilite după
Lippincott Williams & Wilkins, a Wolters Kluwer
detorsiunea chirurgicală, practicându-se predominant la
business; pag. 1642.
pacientele tratate prin laparotomie.
4.
US National Library of Medicine, National Institutes
De-a lungul ultimilor 20 de ani, comparativ cu
of Health. Pelvic in ammatory disease (PID). http://
laparotomia, laparoscopia a demonstrat în mod constant
scăderea pierderii de sânge intraoperator, scăderea
htm.
formării de aderen e, reducerea perioadei de spitalizare, a
5.
Anjali Agrawal, MD. Imaging in Pelvic In ammatory
durerii post-operatorii și a perioadei de recuperare
Disease and Tubo-Ovarian Abscess. Available at http://
postoperatorie, permi ând pacientei să revină mai repede
emedicine.medscape.com/article/404537-overview.
la activitatea normală [2,3]. Studiul de fa ă demonstrează
6.
Avan BI, Fatmi Z, Rashid S. Comparison of clinical
și el tocmai acest fapt: timpul de operare a fost în medie
and laparascopic features of infertile women su ering
de 90,81 minute pentru laparoscopie și 81,16 minute
from genital tuberculosis (TB) or pelvic in ammatory
pentru laparotomie; pierderea de sânge intraoperator a
disease
(PID) or endometriosis. J Pak Med Assoc
fost semni cativ mai scăzută în lotul pacientelor tratate
2001;51(11):393-9.
laparoscopic, comparativ cu cele tratate prin laparotomie;
7.
Heaton FC, Ledger WJ. Postmenopausal tuboovarian
morbiditatea postoperatorie a fost prezentă în propor ie
abscess. Obstet Gynecol 1976;47(1):90-4.
de 5,81% la pacientele tratate laparoscopic și 7,97% la
8.
Champion JD, Piper J, Shain RN, Perdue ST,
cele tratate prin laparotomie; pacientele tratate
Newton ER. Minority women with sexually transmitted
laparoscopic au prezentat cistită postoperator, iar cele
diseases: sexual abuse and risk for pelvic in ammatory
tratate prin laparotomie s-au complicat postoperator cu
disease. Res Nurs Health 2001;24(1):38-43.
infec ia plăgii operatorii și infec ia pelvică. Trei paciente
9.
Koumans EH, Kendrick JS. Preventing adverse sequelae
au necesitat transfuzie după o sarcină ectopică ruptă, una
of bacterial vaginosis: a public health program and
tratată laparoscopic și două tratate prin laparotomie,
research agenda. Sex Transm Dis 2001;28(5):292-7.
132
Babău et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
ORIGINAL ARTICLES
10.
Ness RB, Hillier SL, Kip KE, et al. Bacterial vaginosis
18.
Lok IH, Sahota DS, Rogers MS, Yuen PM.
and risk of pelvic in ammatory disease. Obstet Gynecol
Complications of Laparoscopic surgery for benign
2004;104(4):761-9.
ovarian cyst. J Am Assoc Gynecol Laparosc 2000;7(4):
11.
Bouyer J, Coste J, Shojaei T, et al. Risk factors for
529-34.
ectopic pregnancy: a comprehensive analysis based on a
19.
Mettler L, Semm K Shiver K. Endoscopic management
large case-control, population-based study in France. Am
of adnexal masses. JSLS 1997;1:103-12.
J Epidemiol 2003;157(3):185-94.
20.
Nezhat CR, Kalyoncu S, Nezhat CH, Johnson E,
12.
Vicken P Sepilian, Reproductive Endocrinology and
Berlanda N, Nezhat F. Laparoscopic management of
Infertility, CHA Fertility Center. Ectopic Pregnancy.
ovarian dermoid cyst: ten years’ experience. JSLS 1999;3
Available
at
(3):179-84.
article/2041923-overview#aw2aab6b2b3aa
21.
Descargues G, Tinlot-Mauger F, gravier A, Lemoine
13.
C William Helm. Ovarian cyst. Available at http://
JP, Marpeau L. Adnexal torsion: a report on forty- ve
emedicine.medscape.com/article/255865-
cases. Eur J Obtet gynecol Reprod Biol 2001;98(1):91-
overview#a0156
6.
14.
Shelton JD. Risk of clinical pelvic in ammatory disease
22.
Shalev E, Peleg D. Laparoscopic treatment of adnexal
attributable to an intrauterine device. Lancet
torsion. Surg Gynecol Obstet 1993;176(5):448-50.
2001;357(9254):443.
23.
Cohen SB, Oelsner G, Seidman DS, Admon D,
15.
Workowski KA, Berman SM. Sexually transmitted
Mashiach S, Goldenberg M. Laparoscopic detorsion
diseases treatment guidelines, 2006. Centers for Disease
allows sparing of the twisted ischemic adnexa. J Am
Control and Prevention MMWR Recomm Rep.
Assoc Gynecol Laparosc 1999;6(2):139-43.
2006;55(RR-11):1-94.
24.
Oelsner G, Cohen SB, Soriano D, Admon D,
16.
Kelly EK, Rudinsky SW. Intrauterine contraception:
Mashiach S, Carp H. Minimal surgery for the twisted
current evidence-based recommendations. J Midwifery
ischaemic adnexa can preserve ovarian function. Hum
Womens Health 2007;52(5):505-7.
Reprod 2003;18(12):2599-602.
17.
Meirik O. Intrauterine devices - upper and lower genital
25.
Oelsner G, Shashar D. Adnexal torsion. Clin Obstet
tract infections. Contraception 2007;75(6 Suppl/):S41-7.
Gynecol 2006;49(3):459-63.
Comparison Between the Classic Surgical Methods and the Laparoscopic Ones in the Benign Tubo-Ovarian Pathology
133
Photos from Medical Days of Satu Mare, 11th Edition
GENERAL REVIEW
TRANSFERUL DE CELULE DE ADOPȚIE O NOUĂ SPERANȚĂ PENTRU
PACIENȚII CU MELANOM METASTAZAT. O REVISTĂ A LITERATURII
Golan Bubis1, Călin Bumbulu2, Lea Rath-Wolfson3
1Facultatea de Biologie, Universitatea Ebraică din Ierusalim, Israel, 2SCM dr. Bumbulu -dr. Balaj, Satu Mare, România,
3Departamentul de Patologie, Spitalul Hasharon, Petah Tikva, a liat la Facultatea de Medicină Sackler, Universitatea
Tel Aviv, Israel
Titlul scurt: transferul de celule de adop ie, melanom metastatic
Adresa pentru coresponden ă:
Golan Bubis
E-mail: bubisgolan@gmail.com
Primit: 15.07.2014
Acceptat: 20.08.2014
Med Con October 2014 Vol 9, No 3, 135-138
Rezumat
strategii împotriva melanomului metastazat. Ea are
poten ialul de a stabiliza și chiar vindeca boala. Pe
Unul dintre cele mai noi tratamente în melanomul
măsură ce tehnicile sunt simpli cate, această terapie
metastazat este transferul de celule de adop ie (adoptive
poate oferită de un număr în creștere de Institute de
cell transfer-ACT) cu limfocite in ltrative tumorale
Cancer.
autologe (autologous tumor in ltrating lymphocytes-
Cuvinte cheie: melanom metastazat, transferul de
TIL), care au capacitatea de a distruge celulele
celule de adop ie, limfocite in ltrative tumorale
melanomului. Scopul acestui articol este de a revizui,
compara și sumariza studiile clinice privind ACT pentru
Introducere
melanomul metastatic. Acest tratament a fost introdus
pentru prima dată la National Institutes of Health.
Pacien ii cu melanom metastazat au o supravie uire
Protocoalele includ un regim de limfodeple ie, cu sau
medie de sub un an [1]. Transferul de celule de adop ie
fără iradiere totală corporală, înainte de perfuzare TIL.
(ACT) folosește limfocite tumorale in ltrative
(TIL)
TIL au fost extrase din melanomul pacientului și apoi
recoltate din tumora pacien ilor, care sunt apoi
multiplicate și reinfuzate acestuia, urmate de doze joase
multiplicate la un număr mare și transferate prin
sau crescute de interleukina-2 (IL-2). S-a demonstrat că
perfuzie înapoi pacientului. Aceste celule au capacitatea
ACT cu TIL a atins răspunsul obiectiv
(RO) în
de a distruge celulele melanomului. Am efectuat o
aproximativ 50% de cazuri și răspuns complet (RC) la
analiză sistematică a studiilor clinice și a studiilor
aproximativ 10% dintre pacien i. În ultimii ani, unele
observa ionale privind tratamentul cu ATC a
simpli cări ale tehnicilor au permis mai multor centre
melanomului metastazat, comparând diferitele
să adopte acest tratament, incluzând centre din Israel,
protocoale și rezultatele clinice.
Danemarca, Suedia și altele.
Transferul de celule de adop ie este o tehnică
Concluzie: imunoterapia ACT este astăzi
promi ătoare, dar consumatoare de muncă. Tumorile
considerată ca ind una dintre cele mai promi ătoare
melanomului metastazat sunt rezecate, tăiate în
Adoptive Cell Transfer - a New Hope for Metastatic Melanoma Patients. A Review
135
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
fragmente mici de 3-5 mm2 și plasate în plăci de cultură
25 mg/m2/zi timp de 5 zile. Două grupuri au primit în
cu mediu de creștere și doze mari (HD) de IL-2. TIL
plus iradiere totală a corpului cu o doză absorbită de 2
sunt ini ial multiplicate timp de 3-5 săptămâni la cel
Gy, sau respectiv de 12 Gy. Acești pacien i au primit,
pu in 50×106 celule. Celulele sunt apoi supuse unui
după perfuzia autologă puri cată de TIL, celule stem
protocol de expansiune rapidă pe parcursul a două
hematopoietice crioconservate CD34+. Pacien ii au avut
săptămâni prin stimularea celulelor T. TIL multiplicate
răspuns complet de
20%-40% și respectiv, o
(la miliarde de celule) sunt spălate, adunate și perfuzate
supravie uire lungă. Totuși, această abordare este prea
pacientului. Aceasta este urmată de una sau două cicluri
toxică și necesită o rezervă de celule stem de ecare dată,
de terapie cu HD IL-2, sau de terapie cu doze mici de
împiedicând aplicarea sa pe scară largă.
IL-2, care sus in persisten a TIL perfuzate in vivo.
TIL tumorale reactive folosite în aceste studii
Înainte de transferul TIL, pacientul este tratat cu un
necesită o durată prelungită de mai multe micro-culturi
regim de pregătire folosind ciclofosfamidă
(Cy) și
și un test individualizat pentru a identi ca recunoașterea
udarabină (Flu), care epuizează tranzitoriu limfocitele
tumorii. Cu toate acestea, mul i pacien i nu au fost în
gazdei, în alte studii ind utilizată suplimentar iradierea
cele din urmă eligibili pentru tratament, deoarece TIL-
corporală totală. Studiile ACT pentru melanom
urile lor nu au trecut testul de recunoaștere a tumorii,
metastazat, sunt prezentate în Tabelul I.
sau progresia bolii a apărut rapid în timpul generării
În 1988 Rosenberg și colab. de la Institutul National
TIL. Astfel, procesul complex de produc ie TIL a fost
pentru Cancer, NIH, Bethesda, Maryland [2] au condus
simpli cat și scurtat, prin generarea de TIL „tinere”
un studiu care includea
20 de pacien i trata i cu
pentru terapie, iar testul de recunoaștere a tumorii,
ciclofosfamidă, urmată 36 ore mai târziu, de perfuzia cu
speci c lotului, a fost eliminat [5].
TIL și doze mari de interleukină-2 (IL-2). Unsprezece
Besser și colab.
[6] de la Sheba Medical Center
pacien i au prezentat o regresie măsurabilă a multiplelor
Israel au recrutat 27 de pacien i cu melanom metastazat,
metastaze. În 2005, Dudley și colab. [3], din același
pentru tratament cu TIL de cultură cu termen scurt.
centru de cercetare a cancerului, au centralizat datele de
Culturile TIL tinere au fost inoculate cu succes la
la
35 de pacien i, având rezultate similare. În 2011,
douăzeci de pacien i (74%), procent care a fost mai
Rosenberg și colab. [4] au rezumat rezultatele de la 93
mare decât cel din protocolul tradi ional. Zece pacien i
de pacien i care au primit diferite protocoale de
au prezentat răspuns clinic obiectiv, doi prezentând
limfodeple ie înainte de perfuzie cu TIL, to i pacien ii
regresie completă a tumorii. În 2013, un grup mai mare
primind un regim de limfodeple ie constând din
de pacien i a fost raportat, cu rezultate statistice similare
ciclofosfamidă 60 mg/kg/zi timp de 2 zile și udarabină
[7].
Tabelul I. Prezentare generală a studiilor ACT: protocoale și rezultate
Răspunsul
Institutul
Nr. pa-
Răspuns
Autor
Anul
clinic
Protocol
Statul/ ara
cien ilor
complet**
obiectiv*
Rosenberg [2]
1988
NIH Maryland
20
11 (55%)
0
TIL, IL-2 HD
Dudley [3]
2005
NIH Maryland
35
18 (51%)
3 (8.6%) TIL tinere, IL-2 HD
Besser [6]
2010
Sheba Medical Center Israel
20
10 (50%)
2 (10%) TIL tinere, IL-2 HD
43
21 (48%)
5(12%)
TIL, IL-2 HD
TBI 2 Gy
25
13 (52%)
5 (20%)
Rosenberg [4]
2011
NIH Maryland
TIL, IL-2 HD
TBI 12 Gy
25
18 (72%)
10 (40%)
TIL, IL-2 HD
Radvanyi [8]
2012
M D Anderson Texas
31
15 (48.4%)
2 (6.5%)
TIL, IL-2 HD
Copenhagen University
TIL, IL-2 doză
Ellebaek [11]
2012
6
4 (66%)
2 (33%)
Denmark
scăzută
Pilon- omas [9]
2012
Mo tt Florida
13
5 (38%)
2 (15%)
TIL, IL-2 HD
TIL, IL-2 doză
Ulenhag [10]
2012
Uppsala University Sweden
23
5 (22%)
1 (4%)
scăzută
Besser [7]
2013
Sheba Medical Center Israel
49
23 (47%)
5 (10.6%) TIL tinere, IL-2 HD
Abrevieri: TIL - Limfocite in ltrative tumorale, IL-2 - interleukina-2, TBI - Iradiere corporală totală, HD - doze mari
* Răspuns complet: dispari ia tuturor metastazelor
** Răspuns clinic obiectiv: a fost observată o scădere cu cel pu in 30% în numărul metastazelor
136
Bubis et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
Rhadvanyi și colab. [8] au prezentat experien a de la
Elve ia, Israel și altele. În prezent, cu toate acestea, nu
MD Anderson cu ACT în melanomul metastazat. Rata
există protocoale ACT aprobate de FDA în SUA, sau de
de succes în realizarea multiplicării TIL a fost de
alte agen ii interna ionale de reglementare, pentru a
aproximativ
62%, indiferent de tipul de tratament
utilizate la pacien ii având cancer.
anterior recoltării tumorale. Ei au avut 48,4% răspuns
Concluzii: Imunoterapia ACT este astăzi
clinic obiectiv și 6,5% răspuns complet.
considerată ca ind una dintre cele mai promi ătoare
Pilon- omas și colab. [9] au raportat rezultatele de
strategii împotriva melanomului metastazat. Ea are
la Mo tt Cancer Center și Institutul de Cercetare din
poten ialul de a stabiliza și chiar vindeca boala. Având în
Tampa, Forida, Statele Unite ale Americii. Au fost
vedere că tehnicile sunt simpli cate, această terapie
înrola i nouăsprezece pacien i,
13 pacien i
(68%)
poate oferită de un număr în creștere de Institute de
nalizând cu succes tratamentul. În rândul pacien ilor
Cancer. Viitorul va decide dacă ACT va progresa de la
trata i a fost atinsă o rată de răspuns global de 38%.
studiile clinice din prezent la tratament aprobat.
Ullenhag și colab.
[10] de la Departamentul de
Oncologie, Radiologie și Știin ele Radia iei, Universitatea
Uppsala, Suedia, au arătat că biopsia cu ac ecoghidată
Referințe
este o abordare sigură și ieftină pentru a ob ine esut
tumoral pentru generarea TIL, mai ales în cazurile în
1.
Tarhini AA, Agarwala SS. Cutaneous melanoma:
care chirurgia este contraindicată. TIL au fost utilizate
available therapy for metastatic disease. Dermatol
er
pentru tratament în asociere cu doze zilnice mici
2006;19(1):19-25.
subcutanate de IL-2. Rata de răspuns a fost ceva mai
2.
Rosenberg SA, Packard BS, Aebersold PM, et al. Use
mică decât în alte centre de cancer, dar încă încurajatoare.
of tumor in ltrating lymphocytes and interleukin-2 in
Ellebaek și colab [11] de la Centrul pentru Terapia
the immunotherapy of patients with metastatic
Imunitară a Cancerului și Hematologie, Spitalul
melanoma. A preliminary report. N Engl J Med
Universitar din Copenhaga, Danemarca, au raportat
1988/319(25):1676-80.
cazurile a 6 pacien i trata i cu rezultate foarte bune. De
3.
Dudley ME, Wunderlich JR, Yang JC, et al. Adoptive
asemenea, ei au utilizat doze mici de IL-2, care au redus
cell transfer therapy following non-myeloablative but
semni cativ toxicitatea terapiei. Un caz de tratament cu
lymphodepleting chemotherapy for the treatment of
TIL a fost, de asemenea, raportat la Centrul de Cercetare
patients with refractory metastatic melanoma. J Clin
Biomedicală, Spitalul nr. 1 din Kunming, Kunming,
Oncol 2005;23(10):2346-57.
Republica Populară Chineză [12]. Joseph și colab. [13]
4.
Rosenberg SA, Yang JC, Sherry RM, et al. Durable
au investigat cele mai bune condi ii pentru succesul
complete responses in heavily pretreated patients with
dezvoltării TIL. Per total, dezvoltarea ini ială a TIL a
metastatic
melanoma using T-cell
transfer
avut succes la 62% dintre pacien i, dar pentru pacien ii
immunotherapy. Clin Cancer Res 2011;17(13):4550-
≤30 de ani ea a fost de 94%. Bio chimioterapia în
7.
intervalul 0-60 zile de la recoltarea tumorii a avut un
5.
Dudley ME, Gross CA, Langhan MM, et al. CD8+
impact negativ ini ial asupra dezvoltării TIL, cu o rată
enriched
„young” tumor in ltrating lymphocytes can
de succes de doar 16% (p<0,0001), fapt care trebuie
mediate regression of metastatic melanoma. Clin Cancer
luat în considerare atunci când se plani că tratamentul
Res 2010;16(24):6122-31.
ACT. Un subcomitet al terapiei cu celule de adop ie a
6.
Besser MJ, Shapira-Frommer R, Treves AJ, et al.
sugerat o abordare privind utilizarea de facilită i
Clinical responses in a phase II study using adoptive
centralizate de expansiune celulară, care vor primi
transfer of short-term cultured tumor in ltration
specimenele și vor expedia produse de perfuzie TIL
lymphocytes in metastatic melanoma patients. Clin
multiplicate centrelor participante, pentru a asigura
Cancer Res 2010;16(9):2646-55.
randamentul maxim și pentru a da produsului
7.
Besser MJ, Shapira-Frommer R, Itzhaki O, Treves AJ,
consisten ă. Dacă va avea succes, această abordare va
Zippel DB, Levy D. Adoptive transfer of tumor-
răspunde de nitiv la întrebarea dacă ACT poate
in ltrating lymphocytes in patients with metastatic
introdusă ca tratament de masă pentru cancer [14].
melanoma: intent-to-treat analysis and e cacy after
Există mai multe studii clinice în curs de desfășurare
failure to prior immunotherapies. Clin Cancer Res
privind tratamentul melanomului prin ACT. Ele pot
2013;19(17):4792-800.
găsite pe ClinicalTrials.gov. Cele mai multe dintre ele
8.
Radvanyi LG, Bernatchez C, Zhang M, et al. Speci c
sunt realizate în Statele Unite ale Americii, dar există, de
lymphocyte subsets predict response to adoptive cell
asemenea, studii în curs în Marea Britanie, Suedia,
therapy using expanded autologous tumor-in ltrating
Adoptive Cell Transfer - a New Hope for Metastatic Melanoma Patients. A Review
137
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
lymphocytes in metastatic melanoma patients. Clin
12. Su X, Zhang L, Wu S, Jin L, Ye J, Guan Z, Chen R.
Cancer Res 2012;18(24):6758-70.
Cascading adoptive cell therapy for metastatic melanoma.
9. Pilon- omas S, Kuhn L, Ellwanger S, et al. E cacy
Cancer Biother Radiopharm 2011;26(3):401-6.
of adoptive cell transfer of tumor-in ltrating lymphocytes
13. Joseph RW, Peddareddigari VR, Liu P, et al. Impact of
after lymphopenia induction for metastatic melanoma. J
clinical and pathologic features on tumor-in ltrating
Immunother 2012;35(8):615-20.
lymphocyte expansion from surgically excised melanoma
10. Ullenhag GJ1, Sadeghi AM, Carlsson B, et al. Adoptive
metastases for adoptive T-cell therapy. Clin Cancer Res
T-cell therapy for malignant melanoma patients with
2011;7(14):4882-91.
TILs obtained by ultrasound-guided needle biopsy.
14. Weber J, Atkins M, Hwu P, Radvanyi L, Sznol M, Yee
Cancer Immunol Immunother 2012;61(5):725-32.
C. Immunotherapy Task Force of the NCI Investigational
11. Ellebaek E, Iversen TZ, Junker N, et al. Adoptive cell
Drug Steering Committee. White paper on adoptive cell
therapy with autologous tumor in ltrating lymphocytes
therapy for cancer with tumor-in ltrating lymphocytes: a
and low-dose Interleukin-2 in metastatic melanoma
report of the CTEP Subcommittee on adoptive cell
patients. J Transl Med 2012;10:169.
therapy. Clin Cancer Res 2011;17(7):1664-73.
138
Bubis et al
GENERAL REVIEW
TRATAMENTUL LAPAROSCOPIC ÎN CANCERUL RECTAL. UNDE
SUNTEM ÎN 2014?
George Dejeu, Adrian Maghiar, Teodor Maghiar, Dan Ciurtin, Marius S rlea, Codru a Macovei
Clinica Chirurgie a Spitalului Pelican din Oradea, România
Adresă pentru coresponden ă:
Dejeu George
Spitalul Pelican Oradea, Str. C. Coposu nr 2, cod 410469, Oradea, jud. Bihor, România
Email: dejeu.george@gmail.com
Primit: 22.08.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 139-142
Rezumat
J. Marks putem asemăna chirurgia laparoscopică a
cancerului rectal cu cel mai înalt munte de escaladat în
Adoptarea proctectomiei laparoscopice pentru
chirurgia laparoscopică [1].
cancer rectal a fost lentă, în primul rând din cauza
Cancerul rectal rămâne o boală di cil de tratat, dar
di cultă ii tehnice a procedurii. Variabilitatea mare de la
odată cu apari ia chirurgiei minim invazive (MIS) sunt
chirurg la chirurg în supravie uirea fără boală și recidivă
disponibile mai multe op iuni pentru pacien i. Boala
pelviană locală după proctectomie deschisă, se datorează
afectează în Statele Unite ale Americii aproximativ
probabil diferen elor de tehnică chirurgicală. Aceste
39.000 de pacien i pe an [2]. Tratamentul cancerului
diferen e sunt susceptibile de a
ampli cate atunci
rectal este o categorie separată de tratamentul cancerului
când la procedură se adaugă provocarea laparoscopiei.
de colon, deși o mare parte din datele disponibile se
Datele despre rezultatele oncologice și func ionale în
referă la ambele localizări, iar problemele legate de
urma proctectomiei laparoscopice sunt limitate. Deși
utilizarea chirurgiei minim invazive se suprapun.
adoptarea de tehnici laparoscopice pentru a executa
Rezec ia minim invazivă pentru cancer rectal a fost
proctectomie curativă se va extinde probabil pe măsură
dovedită a fezabilă, iar selec ia pacien ilor depinde atât
ce provocarile tehnice vor
depășite, experien a și
de caracteristicile tumorale, cât și de factorii speci ci
pregătirea se vor îmbunătă i. Sunt necesare studii
pacientului [3,4]. Rezec ia unui cancer rectal implică
multicentrice prospective pentru a ne asigura că
luarea în considerare a stadiului tumorii, nivelului
procedurile furnizează rezultatul oncologic și func ional
tumorii în rect, implicării mezorectale și a invaziei locale
echivalent interven iilor chirurgicale clasice.
a organelor adiacente [5].
Cuvinte cheie: laparoscopie, cancer rectal,
Cel mai important factor pentru orice opera ie de
proctectomie
cancer rectal ar trebui să e în mod evident rezultatul
oncologic. Standardul de îngrijire trebuie să se bazeze pe
Cancerul rectal rămâne o problemă chirurgicală
supravie uirea pe termen lung. Cu toate acestea,
comună și complexă. Există tot mai multe dovezi ale
ob inerea acestor date necesită o urmărire postoperatorie
chirurgiei minim invazive care pot oferi îngrijirea ideală
a pacien ilor lungă și costisitoare. O parte din ob inerea
pentru pacien ii având cancer rectal. Parafrazându-l pe
unui bun rezultat oncologic în tratamentul cancerului
Laparoscopic Treatment in Rectal Cancer. Where Are We in 2014?
139
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
rectal este respectarea principiilor exciziei totale de
reper sunt rezultatele clinice ale studiului clinic COST
mezorect (TME) [6-8]. Acest lucru a fost stabilit în mod
(Clinical Outcomes of Surgical erapy), care a extins
clar în literatura de specialitate ca ind cea mai bună
tendin a aplicării tratamentului laparoscopic în mod
metodă care conduce la rezultate oncologice bune [9,10].
special a cancerului de colon, cu rapoarte de echivalen e
De ce tratamentul laparoscopic al cancerului rectal
oncologice între abordările deschise și laparoscopice și
este un astfel de demers di cil? Anatomia rectului!
un bene ciu în ceea ce privește obiectivele secundare
Rectul este un organ tubular gros a at în spa iul limitat
pentru grupul laparoscopic [13].
al pelvisului osos, un spa iu îngust. Operatorul are o
Experien a mai bogată ob inută folosind rezec ia
vedere de sus a ceea ce poate comparat cu o pâlnie,
rectală laparoscopică sugerează că rezultatele oncologice
care este ocupată aproape în întregime de rect. Acest
precoce sunt echivalente cu cele ale chirurgiei deschise
lucru face di cilă disec ia, deși planul de disec ie,
[12,14-21]. Sprijinul pentru rezec ia rectală laparoscopică
„planul sfânt” (‘holy plane’) [10], este avascular, și ușor
în tratamentul cancerului rectal primar a fost adus printr-
de găsit. Spa iul redus al bazinului, mai ales într-un
un număr de rapoarte [22,23], studii clinice randomizate
pelvis de sex masculin, face deasemenea di cilă sec iunea
[18,19,24,25] și meta-analize [14,26,27].
rectului distal de tumoră și cu cât tumora este mai joasă,
Deși siguran a și echivalen a oncologică a rezec iei
cu atât este mai di cilă plasarea staplerului într-o pozi ie
laparoscopice rectale comparativ chirurgiei deschise
bună. Toate acestea trebuie să ia în considerare siguran a
rectale au fost în general acceptate, tehnica încă nu este
oncologică, care este de nită cel mai bine de marginea
utilizată pe scară largă. Procedura rezec iei laparoscopice
circumferen ială de rezec ie și marginea distală de
rectale este exigentă din punct de vedere tehnic. Curba
rezec ie. Marjele distale care de neau opera ia ca sigură
de învă are semni cativă, limitele înguste ale pelvisului
din punct de vedere oncologic au scăzut în timp, ind
osos și limitele angulare în tehnologia actuală de staplat,
su cientă în cele mai recente orientări la doar
împreună cu practica standard de salvare a nervilor
aproximativ
1 cm (Ghidul SAGES - al Societă ii
autonomi pelvini în excizia totală mezorectală (TME),
Americane a Chirurgilor Gastroenterologi de Tratament
au făcut mai provocatoare chirurgia laparoscopică
Laparoscopic al Cancerului Rectal). Mai importantă
pentru cancerul rectal
[28]. Tipul corporeal al
este realizarea unei margini de rezec ie circumferen iale
pacientului, invazia locală și al i indicatori pot identi ca
libere
(CRM) de tumoră, la încheierea interven iei
pacien ii nepotrivi i pentru rezec ia laparoscopică rectal,
chirurgicale. Acest lucru înseamnă disec ia în afara a
iar ratele de conversie tind să e mai mari decât pentru
ceea ce oma Ionescu a numit primul „fascia propria”
cancerul de colon.
a rectului în 1894, adică a ceea ce numim acum fascia
SAGES, prin consensul asupra interven iilor
mezorectală.
chirurgicale laparoscopice în cancer rectal din
2006
Mezorect este un cuvânt care a fost folosit, probabil,
precizează:
pentru prima dată de Maunsell în 1892 și mai târziu a fost
„Recomandare - rezec ia laparoscopică pentru cancerul
popularizat de Heald, când se referea la ceea ce este acum
rectal trebuie să respecte principiile oncologice standard de
„standardul de aur” în chirurgia cancerului rectal, excizia
marjă distală adecvată, ligatura arterială de bază a arterei
totală de mezorect [6]. Mezorectul este compus din toată
rectale/superioară a arterei mezenterice inferioare și excizia
grăsimea și nodulii limfatici, care sunt incluși în fascia
mezorectală (Nivel II dovezi, gradul B de recomandare);
mezorectală (“fascia propria” a rectului), până la mușchiul
O marjă distală de 1-2 cm;
pubo-rectalis. Excizia totală de mezorect presupune
Eliminarea aportului de sânge și limfatice până la
disec ia completă și excizia, în bloc cu tumora, rectul și
originea arterei rectale superioare (sau arterei mezenterice
vasculariza ia sanguină și limfatică, cu toată grăsimea și
inferioare, dacă este indicat) și excizia totală a mezorectului
ganglionii limfatici închiși în interiorul fasciei mezorectale,
cu margini radiale libere;
deci tot mezorectul până la mușchii ridicători anali.
Recomandare: o formare profesională adecvată și
Se poate face acest lucru laparoscopic? Este di cil,
experien ă sunt necesare pentru a efectua o rezec ie
dar se poate face, și de fapt, aceasta se face cu succes în
oncologică adecvată (Nivel II, Grad B)” [11].
întreaga lume. Laparoscopia s-a folosit pentru chirurgie
EAES
(Asocia ia Europeană pentru Chirurgie
colorectală, în ultimul deceniu, pe scară largă. Sunt
Endoscopică și alte Tehnici Interven ionale) la un
dovedite mai multe avantaje ale chirurgiei laparoscopice
consens cu privire la tratamentul laparoscopic al
colorectale, inclusiv dureri postoperatorii mai reduse,
cancerului rectal în 2010 spune:
un ileus postoperator mai scurt, o spitalizare mai scurtă,
„Ca și în chirurgia deschisă, principiile oncologice
rezultate cosmetice superioare și efecte favorabile asupra
(margini de rezec ie, ligatura vaselor mari, limfadenectomia,
citokinelor și răspunsurilor hormonale [12]. Punctele de
etc) ar trebui să e respectate prin abordul laparoscopic
140
Dejeu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
(92,9%
[Consens]; Grad de recomandare B:
92,9%
ca chirurgia robotică a cancerului colorectal este net
[consens]);
superioară laparoscopiei în reducerea ratei de conversie
Scopul principal este o margine de rezec ie liberă de
intraoperatorii, o constatare care este cel mai probabil
tumoră. Ori de câte ori este posibil ar trebui să e ob inută
rezultatul opticii mai bune, instrumentelor articulate și
o marjă liberă de tumoră (92,9% [consens]; Grad de
retrac iei mai sigure. Dacă pentru cancerul colorectal
recomandare B: 85.7% [consens]);
chirurgia robotizată va îmbunătă i rezultatele pe termen
Disec ia pelvină și mobilizarea rectală trebuie să e
lung, cum ar cele ale func iei sexuale și urinare, rămâne
făcute de o persoană cali cată, în conformitate cu
încă neclar. Deoarece utilizarea chirurgiei robotice
principiile TME
([Consens puternic]
100%; Grad de
crește, evaluarea critică a rezultatelor este de o importan ă
recomandare A: 92,1% [consens]);
vitală, nu numai pentru a preveni daune nejusti cate
Consens cu privire la cancerul rectal tratament
pacien ilor, dar, de asemenea, pentru a controla
laparoscopic 2010: Abordarea laparoscopica a TME nu este
provocările nanciare considerabile pe care le prezintă
inferioară celei deschise
(clasice) din punct de vedere al
această tehnologie scumpă, nouă, în epoca noastră de
supravie uirii fără boală, în supravie uirea globală sau în
creștere a costurilor de îngrijire a sănătă ii. Sunt necesare
recidivele locale (92,9% [consensul]; Grad de recomandare
studii suplimentare randomizate de înaltă calitate pentru
B: 85,7% [consens])” [29].
a determina avantajele reale și neajunsurile chirurgiei
Cum rămâne cu robotul?
robotice minim invazive, pentru cancer rectal.
Utilizarea tehnologiei minim invazive a avut un
Chirurgia minim invazivă pentru cancer rectal are
impact semni cativ asupra interven iei chirurgicale
poten ial. Primele date sugerează îmbunătă irea rezultatelor
colorectale și în ecare an aduce noi aplica ii [30]. Cu toate
pe termen scurt și nu în detrimentul rezultatelor
acestea, chirurgia laparoscopică are limitări. Instrumentele
oncologice. Sunt în curs de desfășurare studii clinice
sunt rigide, limitând mișcările chirurgului, iar acest lucru
randomizate multi-institu ionale. Educa ia și acordarea
poate un dezavantaj semni cativ atunci când operează în
competen elor chirurgilor pentru tehnicile minim invazive
limitele înguste ale pelvisului. În plus, ajutorul chirurgului
pentru tratamentul cancerului rectal ar trebui să asigure
trebuie să aibă o experien ă considerabilă pentru a oferi o
adoptarea de tehnici oncologice adecvate și să ducă la
vizualizare stabilă și o retrac ie tisulară stabilă. Aceste
rezultate oncologice corespunzătoare, presupunând că
aspecte rezultă într-o curbă de învă are abruptă; un studiu
datele viitoare con rmă chirurgia minim invazivă ca o
a estimat că adevărata competen ă se realizează numai
metodă adecvată pentru a trata cancerul rectal.
după 50 de cazuri operate [31].
De la începutul anilor
2000, utilizarea unei
platforme robotizate chirurgicale a devenit tot mai
Referințe
populară. Tehnologia robotică poate ajuta la depășirea
unora dintre limitarile chirurgiei colo-rectale
1. Marks J. Laparosopic surgery in rectal cancer, can it be
laparoscopice [32]. Instrumentele chirurgicale robotice
done? SAGES 2013, Colorectal MIS Postgraduate
sunt exibile și manevrabile, oferind mișcare articulată.
Course, Baltimore MA.
Acest lucru permite chirurgului să ajungă în jurul unor
2. Jemal A, Siegel R, Xu J, Ward E. Cancer statistics,
structuri anatomice, să func ioneze în spa ii mici și să
2010. CA Cancer J Clin 2010;60(5):277-300.
efectueze disec ie laterală precisă. Camera robotică oferă
3. Leroy J, Jamali F, Forbes L, et al. Laparoscopic total
o vedere de înaltă de ni ie tridimensională
(3D),
mesorectal excision
(TME) for rectal cancer surgery:
montată pe un bra robotic, este stabilă și controlată de
long-term outcomes. Surg Endosc 2004;18(2):281-9.
către chirurgul operator.
4. Lujan J, Valero Q, Hernandez A, et al. Randomized
În cele din urmă, s-a estimat că după aproximativ 20
clinical trial comparing laparoscopic and open surgery in
de cazuri curba de învă are este atinsă chiar și de medicii
patients with rectal cancer. Br J Surg 2009;96(9):982-
care nu au experien ă laparoscopică semni cativă [33].
9.
Pentru că robotul permite îmbunătă irea vizualizării și
5. Bleday R, Brindzei N. Surgical treatment of rectal
manipulării, facilitând disec ia precisă în limitele
cancer.
e ASCRS textbook of colon and rectal
bazinului osos, utilizarea rezec iei robotic-asistată pentru
surgery, 2011;731-41.
pacien ii având cancer rectal este în creștere.
6. Heald RJ, Husband EM, Ryall RD. e mesorectum
Rolul roboticii în chirurgia cancerului colorectal
in rectal cancer surgery-the clue to pelvic recurrence? Br J
este încă în curs de de nire. Tehnologia robotică
Surg 1982;69(10):613-6.
demonstrează o mare promisiune, iar studiile de până
7. MacFarlane JK, Ryall RD, Heald RJ. Mesorectal excision
acum au demonstrat siguran a sa. Unele studii au arătat
for rectal cancer. Lancet 1993;341(8843):457-60.
Laparoscopic Treatment in Rectal Cancer. Where Are We in 2014?
141
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
8.
Quirke P. Training and quality assurance for rectal
22.
Baik SH, Gincherman M, Mutch MG, Birnbaum
cancer:
20 years of data is enough. Lancet Oncol
EH, Fleshman JW. Laparoscopic vs open resection for
2003;4(11):695-702.
patients with rectal cancer: comparison of perioperative
9.
Quirke P, Durdey P, Dixon MF, et al. Local recurrence
outcomes and long-term survival. Dis Colon Rectum
of rectal adenocarcinoma due to inadequate surgical
2011;54(1):6-14.
resection. Histopathological study of lateral tumor spread
23.
Laurent C, Leblanc F, Gineste C, Saric J, Rullier E.
and surgical excision. Lancet 1986;2(8514):996-9.
Laparoscopic approach in surgical treatment of rectal
10.
Heald RJ, Moran BJ, Ryall RD, et al. Rectal cancer:
cancer. Br J Surg 2007;94(12):1555-61.
the Basingstoke experience of total mesorectal excision.
24.
Kang SB, Park JW, Jeong SY, et al. Open versus
Arch Surg 1998;133(8):894-9.
laparoscopic surgery for mid or low rectal cancer after
11.
neoadjuvant chemo radiotherapy
(COREAN trial):
guidelines-for-laparoscopic-resection-of-curable-colon-
short-term outcomes of an open-label randomised
and-rectal-cancer/ accessed on 22/08/2014 15:20 GMT
controlled trial. Lancet Oncol 2010;11(7):637-45.
12.
Leung KL, Lai PB, Ho RL, et al. Systemic cytokine
25.
Ng SS, Leung KL, Lee JF, Yiu RY, Li JC, Hon SS.
response after laparoscopic-assisted resection of recto
Long- term morbidity and oncologic outcomes of
sigmoid carcinoma: a prospective randomized trial. Ann
laparoscopic-assisted anterior resection for upper rectal
Surg 2000;231(4):506-11.
cancer: ten-year results of a prospective, randomized
13.
Clinical Outcomes of Surgical erapy Study Group. A
trial. Dis Colon Rectum 2009;52(4):558-66.
comparison of laparoscopically assisted and open colectomy
26.
Huang MJ, Liang JL, Wang H, Kang L, Deng YH,
for colon cancer. N Engl J Med 2004;350(20):2050-9.
Wang JP. Laparoscopic-assisted versus open surgery for
14.
Anderson C, Uman G, Pigazzi A. Oncologic outcomes
rectal cancer: a meta-analysis of randomized controlled
of laparoscopic surgery for rectal cancer: a systematic
trials on oncologic adequacy of resection and long-term
review and meta-analysis of the literature. Eur J Surg
oncologic
outcomes.
Int
J
Colorectal Dis
Oncol 2008;34(10):1135-42.
2011;26(4):415-21.
15.
Aziz O, Constantinides V, Tekkis PP, et al. Laparoscopic
27.
Ohtani H, Tamamori Y, Azuma T, et al. A meta-
versus open surgery for rectal cancer: a meta-analysis.
analysis of the short- and long- term results of randomized
Ann Surg Oncol 2006;13:413(3)-24.
controlled trials that compared laparoscopy-assisted and
16.
Gao F, Cao YF, Chen LS. Meta-analysis of short-term
conventional open surgery for rectal cancer. J
outcomes after laparoscopic resection for rectal cancer.
Gastrointest Surg 2011;15(8):1375-85.
Int J Colorectal Dis 2006;21(7):652-6.
28.
Row D, Weiser MR. An update on laparoscopic
17.
Lelong B, Bege T, Esterni B, et al. Short-term outcome
resection
for
rectal
cancer. Cancer Control
after laparoscopic or open restorative mesorectal excision
2010;17(1):16-24.
for rectal cancer: a comparative cohort study. Dis Colon
29.
Siegel R, Cuesta MA, Targarona E, et al. Laparoscopic
Rectum 2007;50(2):176-83.
extra peritoneal rectal cancer surgery: the clinical practice
18.
Lujan J, Valero G, Hernandez Q, Sanchez A, Frutos
guidelines of the European Association for Endoscopic
MD, Parrilla P. Randomized clinical trial comparing
Surgery (EAES). Surg Endosc 2011;25(8):2423-40.
laparoscopic and open surgery in patients with rectal
30.
Peterson CY, Weise M R. Robotic Colorectal Surgery. J
cancer. Br J Surg 2009;96(9):982-9.
Gastrointest Surg 2014;18(2):398-403.
19.
Ng SS, Leung KL, Lee JF, Yiu RY, Li JC, Teoh AY,
31.
Li JC, Lo AW, Hon SS, Ng SS, Lee JF, Leung KL.
Leung WW. Laparoscopic-assisted versus open
Institution learning curve of laparoscopic colectomy-a
abdominoperineal resection for low rectal cancer: a
multi-dimensional analysis. Int J Colorectal Dis
prospective randomized trial. Ann Surg Oncol
2012;27(4):527-33.
2008;15(9):2418-25.
32.
Peterson CY, McLemore EC, Horgan S, Talamini
20.
Staudacher C, Vignali A, Saverio DP, Elena O,
MA, Ramamoorthy SL. Technical aspects of robotic
Andrea T. Laparoscopic vs open total mesorectal excision
proctectomy. Surg Laparosc Endosc Percutan Tech
in unselected patients with rectal cancer: impact on early
2012;22(3):189-93.
outcome. Dis Colon Rectum 2007;50(9):1324-31.
33.
Jiménez-Rodríguez RM, Díaz-Pavón JM, de la
21.
Strohlein MA, Grutzner KU, Jauch KW, Heiss MM.
Portilla de Juan F, Prendes-Sillero E, Dussort HC,
Comparison of laparoscopic vs open access surgery in
Padillo J. Learning curve for robotic-assisted laparoscopic
patients with rectal cancer: a prospective analysis. Dis
rectal cancer surgery. Int J Colorectal Dis
Colon Rectum 2008;51(4):385-91.
2013;28(6):815-21.
142
Dejeu et al
GENERAL REVIEW
FIBROZA MIOCARDICĂ, PROCES FIZIOPATOLOGIC ÎN REMODELAREA
CARDIACĂ
Lala I. Radu, Maria Puşchi ă
Facultatea de Medicină, Farmacie şi Medicină Dentară, Universitatea de Vest „Vasile Goldiş”, Arad, România
Adresa pentru coresponden ă:
Radu Lala, Maria Puschi ă
Facultatea de Medicină, Farmacie şi Medicină Dentară
Universitatea de Vest „Vasile Goldiş” din Arad,
Arad, Str. Liviu Rebreanu nr.86
Email: radu_lala@yahoo.com, mpuschita@yahoo.com
Primit: 05.09.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 143-148
Rezumat
insu cien a cardiacă, având la bază modi cări moleculare,
celulare și intersti iale ca rezultat al leziunii miocardice,
Insu cien a cardiacă este un sindrom clinic
activării neurohormonale și a încărcării hemodinamice.
caracterizat prin de cit de pompă, la baza căreia stau
Toate aceste procese vor contribui la modi carea
reorganizarea structurilor normale existente la nivel
structurii și dimensiunii cordului, cu exteriorizarea în
cardiac, proces cunoscut ca „remodelare”. Insu cien a
nal a simptomatologiei speci ce. Miocitul este celula
cardiacă reprezintă principala cauză de spitalizare la
principală suferindă și implicată în acest proces, pe lângă
persoanele vârstnice și este asociată cu o morbiditate și
intersti iul sau vasculariza ia coronariană. Remodelarea
mortalitate crescută. Prevalen a crescută a mortalită ii în
cardiacă presupune procese ischemice, in amatorii, de
insu cien a cardiacă se datorează în special aritmiilor
broză, necroză și apoptoză [1].
maligne și a mor ii subite, atribuite procesului de broză
Atât activarea neuroumorală, cât și cea adrenergică,
miocardică. Deși nu se cunosc pe deplin toate mecanismele
sunt crescute la pacien ii cu insu cien ă cardiacă, acestea
și morfologia implicate în remodelarea ventriculară, în
contribuind semni cativ la evolu ia și prognosticul bolii.
ultimul timp s-a pus accent pe broza miocardică, intens
Angiotensina II este unul dintre mediatorii principali ai
studiată, care stă la baza remodelării cardiace. Etiologia
remodelării cardiace și a cărei produc ie locală este
brozei este multifactorială, precum ischemia, in ama ia,
mediată de întinderea brelor miocardice. Efectul
hipoxia, peptidele vasoactive, procese responsabile și
acesteia este unul proliferativ și de creștere, care se
implicate în apari ia insu cien ei cardiace.
manifestă prin sinteza de ADN la nivelul broblastelor și
Cuvinte cheie: remodelare, broblaste, broză
a proteinelor excesiv la nivel broblastic și miocitar.
Angiotensina II prezintă de asemenea un efect citotoxic
Conceptul de remodelare cardiacă
la nivelul celulelor miocardice, prin activarea exagerată a
în insuficiența cardiacă
sistemului renină-angiotensină-aldosteron în insu cien a
cardiacă
[2-3]. O cale alternativă a generării de
Remodelarea cardiacă reprezintă un proces
angiotensină II la nivel miocardic este calea chimazelor,
ziopatologic determinant al evolu iei clinice în
care are o speci citate mai înaltă de transformare a
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
143
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
angiotensinei I în angiotensina II. Chimazele sunt
formează o re ea în jurul miocitelor, tolerantă la stresul
depozitate în granulele citoplasmatice ale celulelor
mecanic [9]. Fibroblastele joacă un rol important în
mastocitare, a căror densitate crește în insu cien a
patologia remodelării cardiace din infarctul miocardic
cardiacă. Astfel, calea chimazelor este importantă în
sau hipertensiunea arterială [9].
promovarea brozei din insu cien a cardiacă, iar
Efectele negative ale broblastelor asupra cordului
inhibarea acesteia poate reprezenta un poten ial terapeutic
sunt exprimate prin diferen ierea acestora în
în regresia remodelării cardiace
[4]. Destinderea
mio broblaste. Activarea broblastelor, cu dobândirea
miocitului ca urmare a leziunii miocardice va determina
unui fenotip tranzitor cu rol secretor, proliferativ,
creșterea activită ii locale a norepinefrinei, angiotensinei
migrator, este realizată de ac iunea neurohormonală, dar
și a endotelinei, care în schimb vor determina hipertro a
și prin stresul mecanic, mai exact prin întindere [10].
miocitară, sinteza de colagen sub ac iunea aldosteronului
Ac iunea predominantă a angiotensinei II se desfășoară
și a citokinelor, cu formarea de matrice extracelulară, ce
la nivelul receptorilor AT1 exprima i de celulele
va duce la broză miocardică [1]. Pentru a compensa
mio broblastice, cu stimularea sintezei de colagen I, III
de citul de pompă al inimii în urma leziunii miocardice,
și
bronectină
[11]. Endotelina-1 ac ionează asupra
catecolaminele ac ionează direct asupra cardiomiocitelor
mio broblastelor prin intermediul receptorilor ETA și
exercitând un efect cronotrop și inotrop. De asemenea,
ETB de la acest nivel, care va avea drept consecin e
ele prezintă un efect citotoxic prin necroza miocitară
creșterea sintezei de colagen, respectiv reducerea
subendocardică pe care o determină [5].
activită ii colagenazelor [12]. Catecolaminele determină
Componentele principale ale remodelării cardiace
modularea broblastelor cardiace prin stimularea
sunt: cardiomiocitul, proliferarea broblastică, respectiv
secre iei de citokine și a factorilor de creștere de către
mecanismele de apoptoză celulară și degradare a
acestea [9]. Stresul mecanic activează broblastele prin
colagenului. Pe parcursul remodelării cardiace miocitele
intermediul integrinelor, canalelor ionice sau
încep să scadă la număr datorită leziunii cardiace, iar
semnalizării celulare secundare, toate acestea ducând la
cele remanente devin parte a procesului compensator,
creșterea secre iei de proteine matriceale, factori de
prin elongare sau hipertro ere, pentru a men ine debitul
creștere și metaloproteinaze [10].
cardiac în condi ii normale
[1]. Alterarea umplerii
Mio broblastele sunt celule cu proprietă i
ventriculare va determina la nivelul cardiomiocitului
proliferative, migratorii și secretorii, care exprimă
sinteza de proteine contractile, care vor forma noi
proteine contractile cum ar
alfa SMA
(actina
sarcomere a căror organizare va stabili e elongarea, e
musculară netedă). Mio broblastele sunt responsabile
hipertro erea celulei, însă totul la pre ul consumului de
de secre ia unor mediatori ai in ama iei cum sunt
oxigen și energie; se creează astfel un cerc vicios care va
citokinele (TNF alfa-factorul de necroză tumorală, IL-
duce la ischemie miocardică și pierderea în continuare
1, IL-6, TGF-beta), peptide vasoactive (angiotensina II,
de celule miocardice
[6]. Ca răspuns al ischemiei
endotelina-1, factorii atriali natriuretici ANP și BNP),
miocardice proliferarea broblastică va stimula sinteza
hormoni (noradrenalină), a căror concentra ie serică
de colagen, care va determina broza parcelară a
este crescută în remodelarea cardiacă. Func ia acestora
ventriculului, contribuind astfel la remodelare [7].
este alterată sub ac iunea unor stimuli ca întinderea
miocitelor, ischemia sau reperfuzia miocardică, care au
Rolul fibroblastelor în remodelarea
drept consecin ă modi carea turn-over-ului matricei
cardiacă
extracelulare prin creșterea secre iei de metaloproteinaze
(enzime degradante ale colagenului) și mediatori ai
Fibroblastele sunt celulele principale responsabile
in ama iei, respectiv reglarea TIMP (inhibitori tisulari
de secre ia în exces a matricei extracelulare, dar și de
ai metaloproteinazelor) [9].
hipertro a cardiomiocitelor prin mecanisme paracrine
Transformarea fenotipică a
broblastelor în
în remodelarea cardiacă, toate acestea contribuind la
mio broblaste nu se regăsește în miocardul normal, în
scăderea func iei contractile a miocardului
[8].
schimb numărul lor abundă în zonele învecinate ale
Fibroblastele reprezintă
70% din celulele cardiace,
infarctului miocardic, unde prin depunerea și sinteza de
având func ia principală de a secreta proteinele matricei
colagen apare esutul cicatriceal brotic [13]. Odată cu
extracelulare care asigură structura compactă a inimii și
maturizarea cicatricei, mio broblastele vor suferi
transmiterea semnalelor mecanice, chimice și electrice
procesul de apoptoză, cu remanen a predominantă la
între componentele celulare și acelulare de la nivelul
acest nivel a componentelor acelulare (colagen, proteine
cordului. Proteina cea mai importantă dintre
matriceale). Totuși, leziuni repetate ale miocardului vor
componentele matricei extracelulare este colagenul, care
contrabalansa acest proces apoptotic, cu persisten a
144
Radu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
mio broblastelor la nivelul esutului cicatriceal
[14].
nivelul esutului infarctizat s-au găsit broblaste care au
Practic, persisten a în continuare a mio broblastelor va
exprimat antigen speci c monocitar de suprafa ă și
facilita în mod direct broza miocardică, care va duce la
anume CD45, CD11b [25].
remodelare patologică și progresie spre insu cien ă
cardiacă. În modelele experimentale pe șoareci s-a
Fibroza miocardică, veriga esențială
observat persisten a mio broblastelor la nivelul zonei
în insuficiența cardiacă
cicatrizante după luni de zile de la infarct
[15]. De
asemenea, în studiile post-mortem pe subiec i umani,
Majoritatea bolilor cardiace care conduc la dezvoltarea
s-a observat prezen a acestor celule în miocard timp de
de insu cien ă cardiacă sunt asociate cu broza
luni sau ani de zile [16].
miocardică. Fibroza miocardică reprezintă procesul de
Fibroblastele sunt mai mult decât niște simple celule
cicatrizare al miocardului prin acumularea de broblaste
formatoare de colagen; ele au fost denumite celule
și secre ia în exces de matrice extracelulară a acestora, care
santinelă, cu func ie imunomodulatorie locală
[17].
va conduce la modi carea structurii și arhitecturii
Fibroblastele au următoarele func ii: homeostazia
organice a inimii [8]. Acumularea excesivă de matrice
matricei extracelulare, producerea de molecule bioactive,
extracelulară va crește rigiditatea pere ilor inimii, cu
homeostazia vaselor cardiace și electro ziologia cardiacă
inducerea de semnale patologice la nivelul cardiomiocitului
[8]. Toate aceste func ii sunt manifestate ca răspuns la
și progresia spre insu cien ă cardiacă [8].
modi cările care apar în mediul lor înconjurător, pentru
S-au descris două forme de broză miocardică:
a prezerva buna func ionare a inimii. Homeostazia
broza intersti ială reactivă și broza de înlocuire. Prima
matricei extracelulare este manifestată prin secre ia de
variantă a fost observată în modelul de supraîncărcare
colagen brilar tip I și III, cel mai abundent colagen la
presională a ventriculului stâng (hipertensiunea arterială,
nivel miocardic, dar și de colagen tip IV,V,VI, elastină
stenoza aortică), ca răspuns de adaptare la presiunile
sau laminină mai pu in abundente, totul ca răspuns la
crescute exercitate la acest nivel și care evoluează în
ac iunea unor factori de creștere, cytokine, sau stimulare
primă fază fără pierderea de cardiomiocite. Dacă nu se
mecanică [18]. Prin secre ia de molecule bioactive este
va elimina obstacolul generator de presiuni crescute la
controlată proliferarea, apoptoza celulară, respectiv
nivelul ventriculului stâng, în nal, broza reactivă va
contrac iile
celulare.
Fibroblastele pot induce
progresa spre broză de înlocuire, caracterizată prin
angiogeneză din vasele preexistente prin secre ia unor
hipertro e și necroză cardiomiocitară [26]. Cea de-a
factori de creștere vasculară
(VEGF, FGF), fenomen
doua formă și anume broza de înlocuire, este întâlnită
observat în ischemia precondi ionată [19]. Fibroblastele,
în infarctul miocardic ca proces imediat reac iei de
de asemenea, contribuie la electro ziologia cardiacă în
in ama ie și a necrozei celulare [27]. În faza ini ială a
mod normal prin formarea unui strat de matrice
remodelării cardiace, broblastele suferă procesul de
extracelulară, care separă activitatea electrică a unor
apoptoză, ca mai apoi să depășească acest mecanism
grupe de miocite. Acest fenomen a fost observat la
compensator, cu formarea persistentă a colagenului
nivelul inelului valvular bros ce separă activitatea
extracelular ca răspuns la injuria miocardică, cu progresia
electrică a atriilor de ventriculi [20]. S-a demonstrat că
nală spre insu cien ă cardiacă [8]. Efectele nocive ale
broblastele pot cuplate de miocite prin intermediul
sintezei excesive de matrice extracelulară asupra func iei
conexinelor, ceea ce poate determina activarea unor
de pompă a inimii se manifestă în mai multe moduri. Pe
grupuri de miocite separate cu formarea unor circuite de
de o parte are loc o creștere a rigidită ii mecanice cu
reintrare, dar și sincronizarea activită ii cardiomiocitare
disfunc ie diastolică, pe de altă parte, prin dispunerea
a ate la distan ă una fa ă de cealaltă
[21-22].
colagenului printre cardiomiocite, are loc o alterare a
Aproximativ 30% din broblastele activate de la nivelul
cuplării electrice intercelulare, cu perturbarea contrac iei
miocardului își au originea din celule endoteliale care
miocardice, deci a func iei sistolice [28]. De asemenea,
suferă un proces de tranzi ie, denumit tranzi ie
in ama ia și broza perivasculară coronariană vor
mezenchimală endotelială
(TME)
[23]. Celulele
diminua uxul cu oxigen și nutrien i la nivel local, ceea
endoteliale, sub ac iunea unor stimuli ca și hipoxia sau
ce va antrena o creștere a răspunsului de remodelare
TGF-beta, vor dobândi un fenotip broblast-like, cu
cardiacă [29]. Remodelarea brotică presupune ac iunea
pierderea caracteristicelor endoteliale. Aceste celule de
asociată a metaloproteinazelor și a factorilor umorali
tranzi ie contribuie la broza miocardică prin proliferare
(angitensina II, endotelina-1, TGF-beta,TNF-alfa)
broblastică, cu sinteza consecutivă de colagen, respectiv
a a i în număr crescut
[10]. Metaloproteinazele, de
rare erea microvasculară [24]. De asemenea, monocitele
exemplu, sunt considerate factorii principali în
au fost enun ate ca o poten ială sursă prin faptul că la
remodelarea matricei extracelulare post-infarct [30]. În
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
145
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
primă fază, acestea din urmă, prin func ia de degradare
intersti iale [41]. Spre deosebire de modelul hipertensiv
a colagenului brilar intersti ial, vor întrerupe matricea
în care sinteza de colagen este mult crescută, la vârstnici,
colagenică extracelulară, cu creșterea răspunsului
broza se datorează în mod principal reducerii activită ii
in amator, ce va atrage după sine proliferare și
metaloproteinazelor care sunt inhibate de inhibitorii
diferen iere broblastică [10].
tisulari ai metaloproteinazelor
(TIMP) sub ac iunea
La nivel electro ziologic
broza miocardică
stimulatoare a TGF-beta [40]. În mod practic este vorba
reprezintă un obstacol în răspândirea normală a excita iei
despre o reducere a degradării matriceale. Deși disfunc ia
prin crearea unui mediu local anizotrop, care predispune
diastolică are rolul principal în patogeneza insu cien ei
la creșterea aritmogenezei
(formarea blocurilor de
cardiace la bătrâni, totuși remodelarea brotică poate
conducere și a reintrărilor), lucru întâlnit frecvent în
afecta și func ia sistolică prin asocierea unor
hipertro a sau ischemia miocardică [31]. Fibroza poate
comorbidită i ca și hipertensiunea arterială, diabetul
determina brila ie atrială sau ventriculară prin
zaharat, sau cardiopatia ischemică.
modularea formării de postpoten iale precoce, care duc
Cordurile senescente, spre deosebire de cele
la activitate trigger [32-33]. Astfel, broza miocardică
sănătoase, prezintă o reac ie in amatorie post-leziune
determină aritmii nu doar prin mecanism de reintrare,
miocardică mai atenuată, rezultând astfel într-o
dar și prin mecanism trigger, cu creșterea anormală a
vindecare și remodelare cardiacă defectuasă. Într-un
automatismului [34].
experiment pe șoareci s-a demonstrat că la șoarecii mai
Fibroza miocardică este considerată determinantul
în vârstă, post-infarct miocardic, există un răspuns
major al disfunc iei diastolice, dar și a alterării func iei
in amator mult diminuat fa ă de cei tineri. Acesta a fost
de pompă a cordului la pacien ii hipertensivi
[35].
caracterizat printr-o scădere a in ltrării estului
Querejeta și colab. [35, 36], în studiul lor, au demonstrat
infarctizat cu neutro le, macrofage și mio broblaste, o
existen a unei asocieri între acumularea miocardică a
reducere a expresiei de citokine, o fagocitoză defectuasă
brelor de colagen tip I la pacien ii hipertensivi și
a cardiomiocitelor, o matrice extracelulară săracă în
deteriorarea func iei cardiace prin măsurarea serică a
colagen și proteine matriceale, toate acestea având ca și
pro-peptidului carboxi-terminal al procolagenului tip I.
rezultat formarea unei cicatrici cu esut conectiv
Hipertro a miocardică consecutivă hipertensiunii
neancorat [42]. Consecin a imediată este remodelarea
arteriale are la bază
2 mecanisme ziopatologice
cardiacă, cu dilatarea ventriculară și disfunc ie sistolică
importante: hipertro a miocitară și acumularea
severă, ceea ce va crește mortalitatea prin insu cien ă
progresivă de esut bros intersti ial [35-37]. Fibroza
cardiacă, dar și apari ia unor complica ii mecanice de
miocardică predispune la insu cien ă cardiacă, de
genul rupturii miocardice la persoanele în vârstă.
exemplu o creștere de 2-3 ori a volumului frac iei de
Fibroza cardiacă și arterială este frecventă la pacien ii
colagen, determinând disfunc ie diastolică cu păstrarea
cu diabet zaharat și predispune la insu cien ă cardiacă.
func iei sistolice, în schimb, o creștere și mai mare a
În mare parte aceasta se datorează remodelării matricei
volumului frac iei o va altera pe aceasta din urmă [38].
extracelulare sub ac iunea unor procese patologice:
Sughira și colab., respectiv Oshato și colab., au
ischemie, in ama ie, stres oxidative, la care se adaugă
demonstrat asocierea semni cativă a volumului frac iei
glicozilarea produșilor nali
(AGE), ce va afecta
de colagen cu disfunc ia diastolică determinată prin
turnoverul colagenului [43].
ecocardiogra e Doppler la pacien ii hipertensivi [38].
Odată cu înaintarea în vârstă are loc depunerea de
Concluzii
colagen în peretele vascular, perivascular, intersti iul
miocardic, care va avea consecin e prin reducerea
Fără îndoială, remodelarea cardiacă are o relevan ă
complian ei miocardice și vasculare
[39]. Astfel,
clinică deosebită, iar în elegerea mecanismelor
creșterea gradului de broză la persoanele vârstnice va
ziopatologice complexe din spatele acesteia este esen ială
crește rigiditatea miocardică cu apari ia disfunc iei
în găsirea unor inte terapeutice pentru a opri acest
diastolice. Fibroza intersti ială rezultă din depunerea de
fenomen de citar, cu poten ial letal crescut. Fibroza
colagen la nivel peri- și endomisial, pe când broza
miocardică este veriga importantă a remodelării cardiace,
perivasculară rezultă din depunerea colagenului la nivel
iar la baza ei stau celulele broblastice cu func ii motrice
adventiceal al arterelor coronare intramurale
[40].
și secretorii, care modelează arhitectura cordului.
Hipertro a miocardică observată la persoanele vârstnice
În elegerea pe deplin a func ionării acestora rămâne în
este o consecin ă a creșterii rigidită ii vasculare periferice,
continuare o enigmă pentru cercetători; de altfel o
care va atrage după sine încărcarea hemodinamică și care
abordare ce presupune descoperirea de noi markeri
la rândul ei va determina creșterea sintezei de colagen
broblastici rămâne o intă de urmărit și demonstrat.
146
Radu et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GENERAL REVIEW
Con ict de interese: Co- nan are din Fondul Social
12.
Katwa LC. Cardiacmyo broblasts isolated from the site
European prin Programul Opera ional Sectorial Dezvoltarea
ofmyocardial infarction express endothelin de novo. Am
Resurselor Umane 2007-2013.(POSDRU/159/1.5/141531).
J
Physiol
Heart
Circ
Physiol
Co-autorul raportează absen a vreunui suport nanciar cu
2003;285(3):H1132-H1139.
interes comercial.
13.
Sun Y, Weber K T. Angiotensin converting enzyme and
myo broblasts during tissue repair in the rat heart. J
Mol Cell Cardiol 1996;28(5):851-8.
Referințe
14.
Desmouliere A, Redard M, Darby I, Gabbiani G.
Apoptosis mediates the decrease in cellularity during the
1.
Cohn JN, Ferrari R, Sharpe N. Cardiac remodeling--
transition between granulation tissue and scar. Am J
concepts and clinicalimplications: a consensus paper
Pathol 1995;146(1):56-66.
from an international forum on cardiac remodeling.
15.
Sun Y, Weber K T. Infarct scar: a dynamic tissue.
Behalf of an International Forum on Cardiac
Cardiovasc Res 2000;46(2):250-6.
Remodeling. J Am Coll Cardiol 2000;35(3):569-82.
16.
Jugdutt BI. Ventricular remodeling after infarction and
2.
Sadoshima J, Izumo S. Molecular characterization of
the extracellularcollagen matrix: when is enough enough?
angiotensin II-induced hypertrophy of cardiac myocytes
Circulation 2003;108(11):1395-403.
and hyperplasia of cardiac broblasts. Critical role of the
17.
Silzle T, Randolph GJ, Kreutz M, Kunz-Schughart
AT1 receptor subtype. Circ Res 1993;73(3):413-23.
LA. e broblast:sentinel cell and local immune
3.
Sadoshima J, Xu Y, Slayter HS, Izumo S. Autocrine
modulator in tumor tissue. Int J Cancer
release of angiotensin II mediates stretch-induced
2004;108(2):173-80.
hypertrophy of cardiac myocytes in vivo. Cell
18.
Bosman FT, Stamenkovic I. Functional structure and
1993;75(5):977-84.
composition of the extracellular matrix. J Pathol
4.
Matsumoto T, Wada A, Tsutamoto T, Ohnishi M,
2003;200(4):423-8.
Isono T, Kinoshita M. Chymase Inhibition Prevents
19.
Chintalgattu V, Nair DM, Katwa LC. Cardiac
Cardiac Fibrosis and Improves Diastolic Dysfunction in
myo broblasts: A novel source of vascular endothelial
the Progression of Heart Failure. Circulation
growth factor (VEGF) and its receptors Flt-1 and KDR.
2003;107(20):2555-8.
J Mol Cell Cardiol 2003;35(3):277-86.
5.
Swynghedauw B. Molecular mechanisms of myocardial
20.
Zhou B, von GA, Ma Q, Hu YW, Pu WT. Genetic
remodeling. Physiol Rev 1999;79(1):215-62.
fate mapping demonstrates contribution of epicardium-
6.
Francis GS, McDonald KM. Left ventricular
derived cells to the annulus brosis of the mammalian
hypertrophy: an initial response to myocardial injury.
heart. Dev Biol 2010;338(2):251-61.
Am J Cardiol 1992;69(18):3G-7G; discussion 7G-
21.
Kohl P. Heterogeneous cell coupling in the heart: An
9G.
electrophysiological role for
broblasts. Circ Res
7.
Volders PG, Willems IE, Cleutjens JP, Arends JW,
2003;93(5):381-3.
Havenith MG, Daemen MJ. Interstitial collagen is
22.
Rohr S. Role of gap junctions in the propagation of the
increased in the noninfarcted human myocardium after
cardiac
action
potential.
Cardiovasc
Res
myocardial infarction. J Mol Cell Cardiol
2004;62(2):309-22.
1993;25(11):1317-23.
23.
Zeisberg EM, Tarnavski O, Zeisberg M, et al.
8.
Krenning G, Zeisberg EM, Kalluri R. e Origin of
Endothelial-to mesenchymal transition contributes to
Fibroblasts and Mechanism of Cardiac Fibrosis. J Cell
cardiac brosis. Nat Med 2007;13(8):952-61.
Physiol 2010;225(3):631-7.
24.
Krenning G, Moonen JR, van Luyn MJA, Harmsen
9.
Porter KE, Turner NA. Cardiac broblasts: At the heart
MC. Vascular smooth muscle cells for use in vascular
of
myocardial remodeling.
Pharmacol
er
tissue
engineering obtained by endothelial-to-
2009;123(2):255-78.
mesenchymal transdi erentiation (EnMT) on collagen
10.
Camellitia P, Borgb TK, Kohla P. Structural and
matrices. Biomaterials 2008;29(27):3703-11.
functional characterisation of cardiac
broblasts.
25.
Haudek SB, Xia Y, Huebener P, et al. Bone marrow-
Cardiovasc Res 2005;65(1):40-51.
derived
broblast precursors mediate ischemic
11.
Lijnen PJ, Petrov VV, Fagard, R H. Angiotensin II-
cardiomyopathy in mice. Proc Natl Acad Sci USA
induced stimulation of collagen secretion and production
2006;103(48):18284-9.
in cardiac broblasts is mediated via angiotensin II
26.
Isoyama S, Nitta-Komatsubara Y. Acute and chronic
subtype 1 receptors. J Renin Angiotensin Aldosterone
adaptation to hemodynamic overload and ischemia in
Syst 2001;2(2):117-22.
the aged heart. Heart Fail Rev 2002;7(1):63-9.
Myocardial Fibrosis a Pathophysiological Process in Cardiac Remodeling
147
GENERAL REVIEW
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
27.
Hasenfuss G. Animal models of human cardiovascular
35.
Díez J, López B, González A, Querejeta R. Clinical
disease, heart failure and hypertrophy. Cardiovasc Res
aspects of hypertensive myocardial brosis. Curr Opin
1998;39(1):60-76.
Cardiol 2001;16(6):328-35.
28.
Chaturvedi RR, Herron T, Simmons R, et al. Passive
36.
Querejeta R, López B, González A, et al. Increased
sti ness of myocardium from congenital heart disease
Collagen Type I Synthesis in Patients With Heart Failure
and implications
for
diastole.
Circulation
of Hypertensive Origin: Relation to Myocardial Fibrosis.
2010;121(8):979-88.
Circulation 2004;110(10):1263-8.
29.
Kai H, Mori T, Tokuda K, et al. Pressure overload-
37.
Cuspidi C, Ciulla M. and Zanchetti A. Hypertensive
induced transient oxidative stress mediates perivascular
myocardial
brosis.
Nephrol Dial Transplant
in ammation and cardiac brosis through angiotensin
2006;21(1):20-23.
II. Hypertens Res 2006;29(9):711-8.
38.
González A, López B, Querejeta R, Díez J. Regulation
30.
Kelly D, Cockerill G, Ng LL, ompson M, Khan S,
of myocardial brillar collagen by angiotensin II. A role
Samani NJ, Squire IB. Plasma matrix
in hypertensive heart disease? J Mol Cell Cardiol
metalloproteinase-9 and left ventricular remodelling
2002;34(12):1585-93.
after acute myocardial infarction in man: a prospective
39.
Lakatta EG, Levy D. Arterial and Cardiac Aging:
cohort study. Eur Heart J 2007;28(6):711-8.
Major Shareholders in Cardiovascular Disease
31.
Spach MS, Boineau JP. Micro brosis produces electrical
Enterprises Part II: e Aging Heart in Health: Links to
load variations due to loss of side-to-side cell connections: A
Heart Disease. Circulation 2003;107(2):346-54.
major mechanism of structural heart disease arrhythmias.
40.
Frangogiannis NG, Biernacka A. Aging and Cardiac
Pacing Clin Electrophysiol 1997;20 (2 Pt 2):397-413.
Fibrosis. Aging and Disease 2011;2(2);158-73.
32.
Ono N, Hayashi H, Kawase A, et al. Spontaneous
41.
Lakatta, James B. Strait, Edward G. Aging-associated
atrial brillation initiated by triggered activity near the
cardiovascular changes and their relationship to heart
pulmonary veins in aged rats subjected to glycolytic
failure. Heart Fail Clin 2012;8(1):143-64.
inhibition. Am J Physiol Heart Circ Physiol
42.
Bujak M, Kweon HJ, Chatila K, Li N, Ta et G,
2007;292(1):H639-48.
Frangogiannis NG. Aging-related defects are associated
33.
Morita N, Sovari AA, Xie Y, et al. Increased
with adverse cardiac remodeling in a mouse model of
susceptibility of aged hearts to ventricular fibrillation
reperfused myocardial infarction. J Am Coll Cardiol
during oxidative stress. Am J Physiol Heart Circ
2008;51(14):1384-92.
Physiol 2009;297(5): H1594-H1605.
43.
Pitt B, Zannad F. e Detection of Myocardial Fibrosis
34.
Karagueuzian H.S. Targeting cardiac brosis: a new
An Opportunity to Reduce Cardiovascular Risk in
frontier in antiarrhythmic therapy? Am J Cardiovasc
Patients With Diabetes Mellitus? Circ Cardiovasc
Dis 2011;1(2):101-9.
Imaging 2012;5(1):9-11.
148
Radu et al
CASE PRESENTATION
LIMFOM PRIMAR DIFUZ CU CELULE TIP B MARI AL HUMERUSULUI.
PREZENTARE DE CAZ ȘI REVISTĂ A LITERATURII
Oana Pobirci1, Elena Roșca2, Dumitru Decebal Pobirci3, Adela Nichita4
1Sec ia de Reumatologie, Spital Pelican, Oradea, 2Departamentul de Anatomie Patologică, Spital Clinic Jude ean Oradea,
3Sec ia Ortopedie și Traumatologie, Spital „Pop Mircea” Marghita, 4Sec ia Radiologie, Spital „Pop Mircea” Marghita,
România
Adresa pentru coresponden ă:
Dr. Oana Pobirci
E-mail: oanap_30@yahoo.com
Primit: 19.08.2014
Acceptat: 30.09.2014
Med Con October 2014, Vol 9, No 3, 149-152
Rezumat
speci că [3]. Limfomul primar non-Hodgkin al osului
cu celule B (PNHLB) reprezintă sub 5% din tumorile
A at printre tumorile osoase rare, limfomul non-
primare osoase și mai pu in de 1% din limfoamele non-
Hodgkinian cu celule B ocupă un loc binemeritat în
Hodgkin. Deoarece sunt atât de rare, există doar cîteva
aten ia medicului, atât prin di cultatea diagnosticului și a
studii retrospective care au fost publicate și care cuprind
tratamentului speci c, cât și prin timpul de laten ă în
prognosticul și tratamentul speci c
[4]. Criteriile de
manifestarea trăsăturilor clinice. Biopsia, urmată de
diagnostic pentru LPB includ [5]: localizarea primară a
colora ii imunohistochimice, este standardul de aur în
tumorii care are origine în măduva osoasă, fără altă
investiga ii. Prezentarea ce urmează descrie un caz rar de
localizare ca extensie a leziunii identi cată prin examen
limfom non-Hodgkin cu celule B la nivel humeral, primul
imagistic sau zic, nu este identi cat limfom în alt loc
caz raportat în literatura română, după știin a noastră.
timp de 6 luni după depistare, diagnosticul trebuie
Cuvinte cheie: limfom non-Hodgkin, tumori
con rmat prin imunohistochimie și trebuie excluse alte
osoase, imunohistochimie
forme de limfoame secundare ale osului.
LPB este un neoplasm rar care este di cil de
Introducere
diagnosticat și este subclasi cat. În trecut doar câteva
cazuri au fost identi cate prin imunofenotipare cu
În România tumorile osoase reprezintă un procent
anticorpi monoclonali [6].
de 1,5%, urmând ca frecven ă localizărilor genitale,
digestive, respiratorii și de sistem. Limfomul primar al
Prezentarea cazului
osului
(LPB) este un tumoră care se formează din
cavitatea medulară și se manifestă ca o leziune solitară,
Pacientul P.A. în vârstă de 77 ani din mediul urban,
localizată, ce reprezintă aproximativ
3% din toate
se internează în cadrul sec iei acuzând dureri profunde la
tumorile osoase maligne și 1% din limfoamele maligne
nivelul umărului drept, care nu au cedat la antialgice, cu
[1]. LPB a fost descris pentru prima dată de Oberling în
impoten ă func ională secundară marcată la acest nivel.
1928 [2] și este în general o boală extrem de rară, pentru
Din antecedentele personale patologice re inem că
care ghidurile terapeutice nu au stabilit încă o terapie
pacientul are adenom de prostată diagnosticat de 5 ani.
Primary Diffuse Large B-Cell Lymphoma of the Humerus. Case Report and Review of Literature
149
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
A
B
Figura 1. Examenul radiogra c
Figura 2. A. Proliferare difuză de celule de talie mare şi medie într-o stromă broasă,
al articula iei scapulo-humerale
hipocelulară (colora ie HE, X 100). B. Prezen a de celule de talie mare şi medie,
drepte prezintă o zonă de osteoliză
cu citoplasma eozino lă și nuclei veziculoşi, nucleola i (colora ie HE, X400)
la nivelul extremită ii proximale
a humerusului drept, cu distrugere
corticală semni cativă
Examenul zic relevă o stare generală ușor
modi cată,
hipotonie
musculară
generalizată,
hepatomegalie la
1 cm sub rebordul costal, ușoară
sensibilitate la palpare în hipocondrul drept. Articula ia
scapulo-humerală dreaptă este blocată antalgic. Nu s-au
constatat adenopatii periferice. Examenul obiectiv al
celorlalte aparate și sisteme a fost în limite normale.
Biologic s-a constatat prezen a unui sindrom in amator
cu VSH 16 mm/oră, dar cu proteina C reactivă negativă.
Radiogra a pulmonară este în limite normale. Pe
radiogra a umărului drept se descrie o zonă de osteoliză
la nivelul extremită ii proximale humerale drepte de 5/4
Figura 3. Markerul CD 20 prezintă expresie
cm, localizată periferic, cu întreruperea compactei
intens pozitivă a celulelor tumorale într-un
interne la acest nivel (Figura 1).
caz de limfom primitiv cu celule mari
Pe ecogra a abdominală se constată catul cu
de tip B (colora ie CD-20, X40).
dimensiuni moderat crescute, prostata cu dimensiuni de
53/42/36 mm, ușor inomogenă.
excluzându-se astfel metastaza carcinomatoasă.
Pentru elucidarea diagnosticului se intervine
Reac iile negative pentru cei 3 markeri neuroendocrini
chirurgical, practicându-se biopsie exploratorie a
- enolaza neuron speci că- NSE, cromogranina și
forma iunii tumorale din extremitatea proximală a
sinapto zina
- exclud tumora neuroendocrină.
humerusului drept. La examenul histologic al
Markerii CD 20 și CLA pozitivi, precum și morfologia
fragmentului de tumoră, se constată un in ltrat cu
celulară, con rmă diagnosticul de limfom malign non-
celule de mărime medie, rotunde, cu nuclei rotunzi,
Hodgkin cu celule B.
nucleoli mici cu citoplasmă în cantitate mică până la
Cazul se trimite sec iei de Oncologie pentru
moderată, cât și limfocite, celule de talie mare cu
aplicarea tratamentului speci c.
citoplasmă eozino lă și nuclei veziculoși, nucleola i,
într-o stromă broasă, hipocelulară (Figura 2, A și B).
Discuții
Colora iile imunohistochimice efectuate pentru
markerii CD 20 și antigenul comun leucocitar (CLA)
Cazul nostru prezintă, din punct de vedere
au fost pozitive (Figura 3).
imagistic, aspectul unei tumori de humerus. Explorările
Colora iile pentru markerii citokeratinici AE 1 și
imagistice ulterioare efectuate nu decelează adenopatii
AE 3, CK 7, CK 20, TTF-1 (thyroid transcription
sau semne de tumoră malignă la nivelul altui organ.
factor 1) au fost negative pentru toate celulele tumorale,
Având în vedere sediul tumorii, s-a presupus ini ial o
150
Pobirci et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
Tabelul I. Limfom primar de humerus, date din literatură,
[8]. Sus inerea diagnosticului s-a făcut prin examinarea
între anii 1970-2014
clinică, rezonan ă magnetică, scintigra e și investiga ii
Nr.
anatomo-patologice care au inclus examenul histologic
Autor
Anul
ara
cazurilor
și imunohistochimic [9].
De Santis E şi colab.[10]
1987
Italia
1 caz
Revizuind cazurile de limfom non-Hodgkin cu
Pettit CK şi colab. [6]
1990
USA
2 cazuri
celule B de humerus publicate în literatură din anul
Blasius S şi colab. [11]
1992
Germania
6 cazuri
1970 până în prezent, am descoperit un număr de 25 de
Arredondo J şi colab. [12]
1999
USA
1 caz
cazuri, al nostru ind al 26-lea (Tabelul I).
Neben K şi colab. [13]
2001
Germania
1 caz
Moazzam N şi colab. [14]
2002
USA
1 caz
Stemberga V şi colab.[15]
2003
Croa ia
1 caz
Concluzii
Robinson D şi colab. [16]
2003
Israel
1 caz
Bralić M şi colab [17]
2008
Croa ia
1 caz
Examenul histopatologic al limfomului non-
Wong T şi colab. [18]
2008
Taiwan
1 caz
Hodgkin cu celule B reclamă obligatoriu examinarea
Marotta D şi colab. [19]
2008
Italia
1 caz
imunohistochimică cu baterii de markeri pozitivi și
Mondal SK şi colab. [20]
2011
India
1 caz
negativi pentru a diferen ia tumorile primare osoase de
Li ZS şi colab. [21]
2011
China
1 caz
Caporale MF şi colab. [9]
2013
Italia
1 caz
cele metastatice. Diagnosticul tumorilor osoase
Mondello P şi colab. [3]
2014
Italia
1 caz
întotdeauna necesită o cooperare interdisciplinară
Ben Salah H şi colab. [22]
2014
Tunisia
4 cazuri
competentă clinică, radiologică, anatomo-patologică.
Pobirci O şi colab.
2014
România
1 caz
După datele pe care le cunoaștem, acesta este primul
caz descris în literatura medicală română.
tumoră primară osoasă
(osteosarcom), exclusă prin
morfologia celulară. S-a luat în considerare ulterior o
metastază cu sediul la nivel humeral, dar
Referințe
imunohistochimia negativă efectuată pentru citokeratine
(CK 7, CK 20), cât și negativitatea TTF-1, exclud
1.
Singh T, Satheesh CT, Lakshmaiah KC, et al. Primary
posibilitatea unei metastaze de carcinom cu punct de
bone lymphoma: a report of two cases and review of the
plecare pulmonar, gastric, etc.
literature. J Cancer Res er 2010;6:296-8.
Aspectul celulelor tumorale - mici, monomorfe - a
2.
Heyning FH, Hogendoorn PC, Kramer MH, et al.
pus problema diagnosticului diferen ial cu o tumoră
Primary non-Hodgkin’s lymphoma of bone: a
neuroendocrină. S-a efectuat imunohistochimia:
clinicopathological investigation of 60 cases. Leukemia
enolaza neuron speci că, sinapto zina și cromogranina
1999;13:2094-8.
au fost negative, ceea ce au exclus tumora
3.
Mondello P, Mian M, Arrigo C, Pitini V. Primary
neuroendocrină. Markerii antigen comun leucocitar
di use large B-cell lymphoma of the bone: bendamustine
(LCA) și CD 20 ind pozitivi, orientează diagnosticul
and rituximab are able to overcome resistant disease.
spre un limfom osos sau determinări osoase în cadrul
Springerplus 2014;3:342.
unui limfom non-Hodgkin cu celule B la nivel humeral.
4.
Lakshmaiah K, Guruprasad B, Purohit S, Rao S,
Absen a adenopatiilor și a altor determinări în alte
Bishwas S, Lokanath D. Primarynon-Hodgkin’s
organe, pledează pentru limfom non-Hodgkin cu celule
lymphoma of bone: poly-ostotic versus mono-ostotic
B, de humerus.
ubtypes. Ecancermedicalscience 2013;7:330.
Limfomul primar de os este o entitate rară. Pacientul
5.
Mulligan ME, McRae GA, Murphey MD. Imaging
acuză dureri locale, iar mai rar, tume ere la nivelul
features of primary lymphoma of bone. AJR Am J
articula iei afectate. Fracturile patologice ale treimii
Roentgenol 1999;173:1691-7.
proximale femurale sau humerale secundare tumorilor
6.
Pettit CK, Zukerberg LR, Gray MH, et al. Primary
de esut moale sunt bine documentate în literatură; cu
lymphoma of bone. A B-cell neoplasm with a high
toate acestea, limfoamele primare la nivelul fracturii
frequency ofmultilobated cells. Am J Surg Pathol
patologice sunt rare [7]. De asemenea, timpul de laten ă
1990;14(4):329-34.
în manifestarea trăsăturilor clinice ale limfomului osos
7.
Siddiqui YS, Khan AQ, Sherwani M. Pathological
reprezintă o di cultate în diagnosticare, accentuând
Fractures in Primary Non-Hodgkin’s Lymphoma of the
necesitatea unui grad mai ridicat de suspiciune atunci
Bone: A Case Series with Review of the Literature. J
când există o neconcordan ă între aspectele clinice și
Clin Diagn Res 2013;7(3):513-7.
cele histopatologice. Întârzierea în elucidare poate avea
8.
Mika J, Schleicher I, Gerlach U, Adler CP, Uhl M,
consecin e serioase și impune ob inerea unui diagnostic
Knoeller SM. Primary bone lymphomas thought to be
Primary Diffuse Large B-Cell Lymphoma of the Humerus. Case Report and Review of Literature
151
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
osteomyelitis urgently demand a rapid diagnosis in bone
16.
Robinson D, Halperin N, Agar G, Alk D, Rami K.
pathology. Anticancer Res 2012;32(11):4905-12.
Shoulder girdle neoplasms mimicking frozen shoulder
9.
Caporale MF, Gambino GF, Larosa FS, Del Buono A,
syndrome. J Shoulder Elbow Surg 2003;12:451-455.
Di Segni F. Non-Hodgkin’s lymphoma: unexpected cause
17.
Bralić M, Stemberga V, Cuculić D, et al. Primary non-
of shoulder pain. A systematic review of the literature.
Hodgkin’s lymphoma of the humerus presenting as
Muscles Ligaments Tendons J 2013;3(3):236-9.
osteomyelitis. Coll Antropol 2008;32 Suppl 2:229-31.
10.
De Santis E, Di Giovanni C, Pallotta F. Primary
18.
Wong T, Ko JY, Wang FS, Chen YJ, Ma MC. Epstein-
reticulosarcoma of bone (non-Hodgkin’s lymphoma). A study
Barr virus associated extranodal natural killer T cell
of 12 cases. Ital. J OrthopTraumatol 1987;13(4):477-84.
lymphoma of nasal type mimicking pyogenic osteomyelitis
11.
Blasius S, Edel G, Vestring T, Ueda Y, Wuisman P,
of the proximal humerus. Chang Gung Med J
Böcker W, Roessner A. Non-Hodgkin’s lymphoma with
2008;31(3):314-9.
primary osseous manifestation, from the les of the Bone
19.
Marotta D, Sgambato A, Cerciello S, et al. Soft tissue
Tumor Registry of Westphalia. Verh Dtsch Ges Pathol
non-Hodgkin lym phoma of shoulder in a HIV patient:
1992;76:146-50.
a report of a case and review of the literature. World J
12.
Arredondo J, Worland R, Sinnenberg R, Qureshi G.
Surg Oncol 2008;6:111.
Non- Hodgkin’s lymphoma as an unexpected diagnosis in
20.
Mondal SK, Bera H, Biswas PK, Mallick MG. High-
a shoul- der arthroplasty. J Arthroplasty 1999;14:108-
grade plasmablastic neoplasm of humerus in an HIV-
11.
negative patient, which was indeterminate between
13.
Neben K, Werner M, Bernd L, Ewerbeck V, Delling
plasmablastic lymphoma and plasmablastic myeloma. J
G, Ho AD. A man with hereditary exostoses and high-
Cancer Res er 2011;7(2):214-6.
grade non-Hodgkin’s lymphoma of the bone. Ann
21.
Li ZS, Li PF, Wang Z, Huang GS. Primary extranodal
Hematol 2001;80(11):682-4.
soft-tissue
B-cell
lymphoma with abundant
14.
Moazzam N, Malik AA, Potti A. B-cell lymphoma mimicking
immunoglobulin
inclusions
mimicking
adult
multiple myeloma. Leuk Lymphoma 2002;43(9):1869-73.
rhabdomyoma: a case report. J Med Case Rep
15.
Stemberga V, Dobi-Babić R, Bosnar A, et al. Primary
2011;7(5):53.
non-Hodgkin lymphoma of the humerus following
22.
Ben Salah H, Fourati N, Elloumi M, Boudawara T,
traumatic injury: case report. Hematol Oncol 2003;
Frikha M, Daoud J. Localized primary bone lymphoma:
21(3):109-14.
about four cases. Cancer Radiother 2014;18(1):23-7.
152
Pobirci et al
CASE PRESENTATION
REPLANTAREA DEGETELOR AMPUTATE PRIN MECANISME DE
AVULSIE TORSIUNE. CONSIDERAȚII TEHNICE ȘI REZULTATE
FUNCȚIONALE
Doina Prisecari1, Dragoș Zam rescu2, Șerban-Arghir Popescu2, Ioan Lascar2, Alisa Zisman1, Alexei Prisecari3
1Clinica de Chirurgie Plastică și Microchirurgie Reconstructivă, Spitalul Clinic Jude ean de Urgen ă „Sf. Apostol Andrei”,
Constan a, România, 2Clinica de Chirurgie Plastică și Microchirurgie Reconstructivă, Spitalul Clinic de Urgen ă
București, Universitatea de Medicină și Farmacie
„Carol Davila” București, Romania,
3Clinica de Ortopedie-
Traumatologie, Spitalul Clinic Jude ean de Urgen ă „Sf. Apostol Andrei” Constan a, România
Adresa pentru coresponden ă:
Prisecari Doina
Spitalul Clinic Jude ean de Urgen ă „Sf. Apostol Andrei”
B-dul Tomis nr 145, CP 900591, Constan a
Tel 0742707124
Email: doinaschipor@yahoo.com
Primit: 02.09.2014
Acceptat: 30.09.2014
Med Con October 2014 Vol 9, No 3, 153-157
Rezumat
Rezultate: au fost implica i
9 pacien i. Rata de
supravie uire a fost de 57% pentru degetele amputate
Amputa iile produse prin avulsie-torsiune constituie
complet și 43% pentru degetele amputate par ial.
o problemă deosebit de complexă întrucât produc leziuni
Cuvinte cheie: avulsie deget, amputa ie deget,
importante la nivelul vaselor și nervilor. Atât anastomoza
rezultatele în chirurgia mâinii, replantare, revascularizare
arterială, cât și anastomoza venoasă, sunt factori
importan i care determină succesul în replantarea
Introducere
degetelor dezmănușate. Experien a chirurgicală în disec ia
vaselor și alegerea procedurii de reconstruc ie folosind
Apari ia tehnicilor de microchirurgie a însemnat un
grefe venoase și nervoase sunt de o importan ă capitală.
mare pas înainte pentru replantarea degetelor amputate
Scopul: urmărirea supravie uirii și a rezultatelor
și dezmănușate. Leziunile produse prin mecanismul de
func ionale în urma replantării digitale după amputarea
dezmănușare constituie o problemă deosebit de gravă și
completă sau incompletă prin mecanismul de dezmănușare.
greu de tratat, întrucât produc leziuni importante atât la
Metode: Criteriile cuprinse în acest studiu au fost:
nivel tegumentar, vascular, cât și la nivel nervos.
amputa ii digitale complete/incomplete la nivelul
Replantarea/revascularizarea unui deget amputat
falangei proximale și distal de articula ia interfalangiană
prin mecanismul de dezmănușare este cea mai solicitantă
proximală; alegerea tratamentului chirurgical de
problemă în chirurgia mâinii, iar eșecul este frecvent.
replantare
sau
revascularizare
- anastomoza
După numeroase replantări în astfel de cazuri, am putea
microchirurgicală arterială, urmată de anastomoza
trage concluzia că replantarea unui segment a avut
venoasă
(prin sutura directă sau grefare venoasă);
succes atunci când vasele de sânge incluse în tegumentul
ob inerea a două puncte de discriminare - echivalent cu
avulsionat nu au avut leziuni supraetajate, sau nu au fost
un rezultat func ional.
distruse ireversibil
(este vorba, de asemenea, despre
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
153
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
circula ia periferică care, în acest tip de traumatism
nervilor și arterelor. Este important să se evite două
determină leziuni ireversibile). Cu toate că degetele
incizii, din cauza riscului crescut de necroză a pielii.
replantate au recuperat su cientă func ie, s-a dovedit a
Arterele și venele sunt marcate pe partea amputată și, de
greu de realizat. Din acest motiv, indica iile și
asemenea, la nivelul bontului. Calitatea vaselor este
contraindica iile pentru pacien ii candida i la opera ie
evaluată la MO, iar capetele sunt sec ionate în esut
au continuat să evolueze pentru excluderea celor cu
sănătos. După xarea oaselor și repararea tendonelor,
prognostic func ional prost de la bun început. Chirurgii
urmează anastomoza arterială, care se realizează cu r
au continuat să extindă limitele de microchirurgie, au
prolene 9.0-10.0. Anastomoza venoasă se face cu r
fost propuse noi tehnici pentru a gestiona di cultă ile și
prolene 10.0-11.0 printr-o tehnică termino-terminală,
salvarea degetelor avulsionate.
sau grefon venos interpus, chiar și când există o mică
Lezunile prin avulsie sunt de obicei citate ca având
tensiune în anastomoză. După reușita anastomozei se
rezultate func ionale precare [1,2,3], mai ales în cazul
practică sutura tegumentară astfel încât să nu existe
amputării complete, sau atunci când există distrugeri de
tensiune.
articula ii interfalangiene
[4,5]. Studiile recente au
prezentat rezultate func ionale bune după replantările de
Rezultate
degete dezmănușate și au contestat această recomandare
[6].
Raportul nostru include un total de 9 cazuri de
Scopul acestui studiu este de a realiza o analiză
amputări prin avulsie-torsiune, dintre care 4 au fost
sistematică a replantărilor degetelor avulsionate, pentru
amputa ii complete și 5 amputatii incomplete. S-au
a oferi cele mai bune dovezi despre ratele de supravie uire
înregistrat 2 eșecuri totale (o femeie și 1 bărbat) și 3
și rezultatele func ionale. Obiectivul secundar a fost de a
cazuri de eșec par ial
(necroze par iale, care au fost
compara rezultatele func ionale după replantarea
rezolvate prin interven ii ulterioare). Un singur pacient
degetelor dezmănușate cu rezultatele ob inute în
a avut nevoie de grefă venoasă în vederea refacerii axului
replantarea degetelor amputate în zona II cu leziuni ale
vascular,
2 pacien i au suferit artrodeză la nivelul
tendoanelor exoare și repararea nervilor digitali.
articula iei interfalangiene proximale și
1 pacient la
Analiza rezultatelor func ionale ob inute prin aceste
nivelul articula iei interfalangiene distale.
două metode constituie un punct de plecare pentru
În toate cazurile s-a anastomozat o singură venă, iar
stabilirea unor protocoale terapeutice.
la 3 cazuri s-a folosit grefa venoasă. Dintre toate cazurile
de succes, doar un pacient a prezentat întoarcere venoasă
Materiale și metode
de citară, motiv pentru care s-au folosit lipitori
medicinale (Figura
3 A,B,C,D,E,F). Niciunul dintre
Scopul acestui studiu a fost să arate că metoda de
pacien i nu a avut nevoie de transfuzie.
replantare sau revascularizare microchirurgicală oferă o
To i pacien ii au fost urmări i la 3, 6 și 12 luni. To i
rată de succes în replantările degetelor avulsionate.
au fost mul umi i de rezultatele func ionale ob inute.
Între anii 2007-2010 au fost replantate 9 degete
Niciunul nu a solicitat amputarea tardivă din cauza
amputate complet sau incomplet prin mecanismul de
aspectului estetic, nevroamelor, rigidită ii, intoleran ei
dezmănușare. Au fost 6 femei și 3 bărba i, cu vârste
la frig.
cuprinse între 26-59 ani. Interven iile s-au realizat sub
Amplitudinea mișcării la nivelul articula iei
anestezie tip bloc digital.
interfalangiene a fost 135º pentru amputa ii complete și
To i pacien ii au fost dreptaci. Degetele afectate au
160º în amputa ii incomplete. Sensibilitatea de protec ie
fost: deget inelar stâng la 4 pacien i, police la 2 pacien i
a fost recuperată în toate cazurile. Fiecare pacient din
(Figura
1 A,B,C,D) și indicele/medius la 3 pacien i
grupul studiat a fost reabilitat social și profesional după
(Figura 2 A,B,C,D).
o perioadă medie de 3-4 luni.
Amputa ii complete la nivelul articula iei
interfalangiene proximale au fost observate în 2 cazuri și
Discuții
1 caz la nivelul articula iei interfalangiene distale.
Drenajul venos a fost realizat printr-o singură anastomoză
Degetele replantate/revascularizate după amputa ie
venoasă (sau grefa venoasă). În toate cazurile anestezia
printr-un macanism de smulgere sunt de obicei citate ca
locală a fost asociată cu un garou la baza degetului. La
având rezultate func ionale rezervate [1,2,3,7], în special
începutul replantării, partea amputată este examinată la
după amputa ie completă, sau atunci când există
microscopul operator
(MO). O incizie longitudinală
distrugeri de articula ii interfalangiene, esuturi moi și
unică se face pe fa a volara a degetului pentru identi carea
pachete vasculonervoase [5,7].
154
Prisecari et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
A
B
C
D
Figura 1. A,B. Dezmănușare totală de police și avulsie de tendon exor lung police
și extensor lung police. C,D. Aspecte la 1 an de zile
A
B
C
D
Figura 2. A,B. Dezmanușare deget II aspect preoperator. C,D. Aspect postoperator
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
155
CASE PRESENTATION
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
A
B
C
D
E
F
Figura 3. A. Femeie cu traumatism prin dezmănușare și amputare completă la nivelul articula iei
interfalangiene a degetului V, cu avulsia exorului profund. B. Artrodeză la nivelul articula iei
interfalangiene a degetului cu broșă axială Kirschner. C,D. Aspect postoperator. E. Aspect la 72 ore-
pacienta a prezentat întoarcere venoasă di citară, pentru care s-au folosit lipitori. F. Aspect la 3 luni
În cazurile în care s-au folosit grefe venoase în
În majoritatea cazurilor, recuperarea func ională este mai
vederea restabilirii axului vascular, permeabilitatea
redusă, iar complica iile sunt mai numerase. Regenerarea
anastomozei a necesitat uneori revizuirea. Această
nervoasă este aproape nulă, mecanismul ind unul de
metodă simplă, rapidă și ușoară a permis vizualizarea
smulgere și elongare a nervilor. În timp, pacien ii dezvoltă
grefelor răsucite, îndoite.
un grad de sensibilitate numită sensibilitate de protec ie.
Grefele de nerv, venă, tendon, permit ob inerea
Din punct de vedere al func ionalită ii, gradul de mișcare
rezultatelor func ionale bune chiar și în cazurile de
activă și pasivă se recuperează în propor ie de până la 50%.
amputare prin dezmănușare. Recoltarea de venă subcutană
Chiar dacă recuperarea func ională este de citară,
în aceste cazuri a reprezentat o tehnică simplă și rapidă [4].
păstrarea degetului reprezintă un factor important în
men inerea calită ii ve ii pacientului, în special pentru
Concluzii
copii și pacien ii de sex feminin.
Utilizarea pe scară largă a grefelor venoase în vederea
Prognosticul în cazul replantărilor degetelor
refacerii axului vascular în cazul traumatismelor prin
dezmănușate în genereal este destul de rezervat comparativ
dezmănușare sau amputare completă, crește rata de
cu cel dat în cazul amputărilor prin mecanisme de tăiere.
succes și se pastrează lungimea degetelui.
156
Prisecari et al
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
CASE PRESENTATION
Având în vedere severitatea traumatismului,
4. Adani R, Marcoccio I, Castagnetti C, Tarallo L. Long-
majoritatea pacien ilor necesită proceduri secundare.
term results of replantation for complete ring avulsion
amputations. Ann Plast Surg 2003;51:564-8.
5. Urbaniak JR, Evans JP, Bright DS. Microvascular
Referințe
management of ring avulsion injuries. J Hand Surg Am
1981;6:25-30.
1. Boulas HJ. Amputations of the ngers and hand:
6. Akyurek M, Safak T, Kecik A. Ring avulsion
indications for replantation. J Am Acad Orthop Sur
replantation by extended debridment of the avulsed
1998;6:100-5.
digital artery and interposition with long venous grafts.
2. Pederson WC. Replantation. Plast Reconstr Surg
Ann Plast Surg 2002;48(6):574e81.
2001;107:823-41.
7. Ross DC, Manktelow RT, Wells MT, Boyd JB.
3. Urbaniak JR, Roth JH, Nunley JA, Goldner RD,
Tendon function after replantation: prognostic factors
Koman LA. e results of replantation after amputation
and strategies to enhance total active motion. Ann Plast
of a single nger. J Bone Joint Surg Am 1985;67:611-9.
Surg 2003;51:141-6.
Replantation of Amputated Fingers After Ring Avulsion. Technical Considerations and Functional Prognosis Results
157
Photos from Medical Days of Satu Mare, 11th Edition
HISTORY OF MEDICINE
CONSTANTIN STANCA 1889 1969 UN GINECOLOG ȘI ONCOLOG
PRESTIGIOS AL SECOLULUI AL XX LEA
Cristian D. Barsu
Disciplina de Ştiin e Socio-Umaniste şi Istoria Medicinii, Universitatea de Medicină şi Farmacie „Iuliu Ha ieganu”,
Cluj-Napoca
Adresa pentru coresponden ă:
Dr. Cristian D. Barsu
Strada Avram Iancu nr 31, CP 400083, Cluj-Napoca, România
Email: cristianbarsu@yahoo.com
Primit: 14.08.2014
Acceptat: 15.09.2014
Med Con October 2014, Vol 9, No 3, 159-162
Rezumat
medicinii românești, în special în prima jumătate a
veacului al XX-lea. El a fost primul director al
Dr. Constantin Stanca
(1889-1969) a fost o
Institutului pentru Studiul și Pro laxia Cancerului,
personalitate prestigioasă în ginecologia și oncologia
(ulterior denumit Institutul Oncologic) din Cluj, între
românească a secolului al XX-lea. El a fost primul director
anii 1929 și 1940. Acesta fusese creat la ini iativa Prof.
al Institutului pentru Studiul și Pro laxia Cancerului din
Dr. Iuliu Moldovan (1882-1966), care în 1929 a fost și
Cluj, între anii 1929 și 1940. Acolo a întemeiat și a condus
directorul său onori c. Institutul a fost o premieră în
Sec ia de Chirurgie ginecologică oncologică. La același
România și unul dintre primele trei institute de
Institut, el a creat Sec ia de Radioterapie și Laboratorul de
specialitate din Europa. Este important să men ionăm
Cancer experimental. O altă reușită a sa a fost fondarea
faptul că până în
1947 Institutul se numea
„Iuliu
primei reviste de cancerologie din România, intitulată
Maniu”, deoarece în 1929 Iuliu Maniu (1873-1953), ca
„Cancerul”, care a existat din 1932 până în 1938. În plus,
prim ministru al României a sprijinit fondarea acestuia.
el a realizat primul lm românesc pe tema cancerului, care
În Institut, C. Stanca a întemeiat Sec ia de Chirurgie
a fost lmat în cadrul Institutului pe care-l conducea. C.
ginecologică oncologică, Sec ia de Radioterapie și
Stanca a fost fondatorul unei importante școli de oncologie
Laboratorul de Cancer experimental, acestea ind
și ginecologie din Transilvania, caracterizată prin
deosebit de moderne pentru nivelul medical interbelic.
profesionalism, elegan ă, radicalism chirurgical și care, în
Lucrarea de fa ă marchează 85 de ani de la în in area
perioada interbelică, a avut rezultate deosebit de bune.
Institutului Oncologic din Cluj.
Cuvinte cheie: Constantin Stanca, ginecologie,
oncologie, Institutul pentru Studiul și Pro laxia
Viața şi cariera lui C. Stanca
Cancerului din Cluj
Constantin Stanca s-a născut la
16 septembrie
Introducere
1889, la Petroșani. El a fost fratele mai mare al lui
Dominic Stanca (1892-1979). Atât ei, cât și unul dintre
Chirurgul ginecolog și oncolog Constantin Stanca
nepo ii lor - Octavian Stanca (1908-1977) - au devenit
(1889-1969) a avut un rol important în dezvoltarea
medici. Este necesar să subliniem faptul că în secolul al
Constantin Stanca (1889-1969) - A Prestigious Gynecologist and Oncologist of the 20th Century
159
HISTORY OF MEDICINE
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
XX-lea - și chiar în prezent - în unele prezentări mai
valoroși din rândul personalului Clinicii de Ginecologie.
persistă încă confuzia între Constantin și Dominic
Acuza ia lui Grigoriu a fost următoarea:
„încălcarea
Stanca.
regulilor de disciplină a Facultă ii și lansarea de informa ii
Conturând istoria familiei Stanca, cunoscutul
false”
[4]. Dacă într-adevăr aceasta a fost numai un
medico-istoric Valeriu Bologa (1892-1971) a eviden iat
pretext, înseamnă că Stanca trebuie să fost apreciat
faptul că aceasta a fost „o familie de cărturari hunedoreni
încă de la debutul carierei sale ca ind un ginecolog de
al căror șir a început cu Stanca-tatăl și a continuat prin i
valoare și având curajul să-și expună punctele de vedere
și nepo i savan i, scriitori și organizatori vajnici în ale
și să suporte consecin ele acestora.
obștii, [familie care] a fost întotdeauna prezentă, timp de
Cariera lui Constantin Stanca a continuat în 1920
optzeci de ani, de câte ori era vorba să se înfăptuiască lucru
în calitate de medic primar la Spitalul de Femei din
bun și trainic pe meleagurile acelei Transilvanii care se
Cluj. Acesta fusese organizat și condus de fratele său
pregătea pentru Unire”
[1]. Pentru a marca într-o
Dominic Stanca, care era și el un ginecolog de valoare.
modalitate mai importantă prestigiul familiei Stanca, V.
Spitalul de Femei din Cluj a fost primul spital
Bologa a adăugat că „în istoriogra e, în medicină și în
ginecologic organizat de Consiliul Dirigent al
literatură, numele de Stanca, timp de trei genera ii, se vede
Transilvaniei imediat după Marea Unire a Transilvaniei
și se aude neîncetat” [1].
cu România.
C. Stanca a fost student al Facultă ii Maghiare de
Fiind avid de dezvoltarea sa profesională, în 1924
Medicină din Cluj. Unul dintre cei mai importan i
Constantin Stanca a devenit docent în ginecologie la
profesori ai săi a fost D. Szabó, care a fost directorul
Facultatea de Medicină din București, având teza:
Clinicii de Ginecologie din Cluj din 1892 până în 1918.
„Direc ii fundamentale în semiologia și propedeutica
Stanca a absolvit facultatea în 1914 și a devenit doctor
obstetricală și ginecologică”. În paralel, timp de opt ani,
în medicină și chirurgie după câteva luni de la absolvire.
din 1921 până în 1929, a fost directorul Sanatoriului de
În același an și-a început cariera didactică la aceeași
Stat de Cruce Roșie din Cluj.
Facultate, la Catedra de Anatomie. Fiind atras de
În aceeași perioadă, el a avut ocazia să-și ampli ce
medicina clinică, la scurt timp el s-a transferat ca asistent
pregătirea profesională la Viena, la Clinica de
la Clinica de Chirurgie din Cluj. Aici a activat până în
Ginecologie condusă de celebrul Prof. Dr. Ernst
1919, când Facultatea Maghiară de Medicină din Cluj
Wertheim
(1864-1920) și apoi de Prof. Dr. Fritz
și-a încetat activitatea.
Kermauner
(1872-1931). De asemenea, Stanca și-a
Este interesant de men ionat faptul că în 12 mai
aprofundat cunoștin ele de tehnică chirurgicală la
1919, Alexandru Nemeș (1891-1973), împreună cu C.
Clinica de Chirurgie din aceeași metropolă, care îl avea
Stanca și Coriolan Tătaru
(1889-1957) au fost
ca director pe Prof. Dr. Anton von Eiselberg (1860-
nominaliza i pentru a membri în grupul care trebuia
1939).
să preia clinicele universitare din Cluj,
„Spitalul
Cea mai importantă parte a carierei lui C. Stanca a
Carolina” și celelalte institute dependente ale vechii
avut loc la Institutul pentru Studiul și Pro laxia
Facultă i de Medicină, pe seama Statului Român.
Cancerului „Iuliu Maniu” din Cluj. Sub conducerea
Această misiune le-a fost dată de Onisifor Ghibu (1883-
Prof. Dr. Iuliu Moldovan, fondatorul Institutului, în
1972) - delegatul Consiliului Dirigent pentru această
1929 C. Stanca a devenit directorul Institutului și a
activitate [2].
adus o contribu ie esen ială la organizarea sa. El a
Apoi, în anul universitar 1919/1920, C. Stanca a
întemeiat Sec ia de Chirurgie ginecologică oncologică,
fost asistent la Clinica de Ginecologie, care atunci
Sec ia de Radioterapie și Laboratorul de Cancer
apar inea de Facultatea Românească de Medicină din
experimental.
Cluj.
O altă realizare a sa a fost întemeierea primei reviste
Ca rezultat al con ictului dintre câ iva asisten i
de oncologie din România. Aceasta a avut titlul
universitari și directorul Clinicii de Ginecologie - Prof.
„Cancerul” și a existat din 1932 până în 1938. La acea
Dr. Cristea Grigoriu (1883-1951), pe 1 aprilie 1920,
vreme era foarte di cil de a crea o revistă specială de
Consiliul Profesoral al Facultă ii de Medicină, condus
oncologie. Această di cultate a avut trei motiva ii.
de decanul Iuliu Ha ieganu (1885-1959), a decis să-i
Prima era faptul că nivelul teoretic al oncologiei nu era
demită pe Alexandru Nemeș și pe Constantin Stanca,
încă foarte dezvoltat. A doua cauză a fost reprezentată de
împreună cu al i trei asisten i [3]. După peste nouă
numărul destul de mic al medicilor din Institutul pentru
decenii de la acest eveniment, este di cil de știut dacă
Studiul și Pro laxia Cancerului din Cluj, care aveau
motiva ia dată de Prof. Grigoriu a fost corectă sau, de
timpul necesar să scrie articole știin i ce bazate pe
fapt, era o scuză pentru a-i elimina pe unii tineri medici
propria lor experien ă în domeniu. Dar, în nal,
160
Barsu
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
HISTORY OF MEDICINE
insu cien a resurselor nanciare a determinat sistarea
Spitalului
„Ilie Pintilie” din București. Acolo a fost
publicării acestei reviste. Având în vedere aceste
director, chirurg ginecolog și obstetrician [8].
considerente, existen a revista „Cancerul” timp de șapte
C. Stanca a reușit să se impună pe linie profesională
ani poate considerată o performan ă pentru medicina
și i s-a acordat titlul de „Profesor Onori c”, apoi, în
din România primei jumătă i a secolului al XX-lea și o
1960 a fost distins cu titlul de „Medic Emerit” [9].
realizare importantă pentru medicina din Europa
Astfel, în anul universitar 1961/1962 a fost profesor de
aceleiași perioade.
obstetrică și ginecologie la Facultatea de Medicină din
Stanca a fost autorul primului lm românesc de
București [10].
oncologie. Acesta a fost realizat în Institutul pe care el îl
Activitatea știin i că a lui Constantin Stanca
conducea și a avut un important rol educativ, atât
include peste
100 lucrări știin i ce, publicate sau
pentru public, cât și pentru medici [5].
comunicate, majoritatea lor având un pro l oncologic.
De-a lungul carierei, el și-a manifestat interesul
Printre acestea sunt incluse următoarele lucrări:
pentru îngrijirea pacien ilor oncologici, cercetarea
„Cancerul tubar primiv”
(1922),
„Noi cercetări în
știin i că, învă ământ și fondarea de unită i oncologice
re exul dureros la distan ă” (1927), „Grefele ovariene”
în arealul Transilvaniei [6].
(1931), „Asupra histerectomiilor totale lărgite pentru
Este important de men ionat faptul că în aceeași
cancerul uterin, pe anii
1924-1935”
(1935),
„La
perioadă în care a fost director al Institutului pentru
connexion pathologique entre le cancer de l’appendice
Studiul și Pro laxia Cancerului din Cluj, C. Stanca și-a
et les ovaires” (1935), „Amputa ia spontană a colului
continuat activitatea la Spitalul de Femei din același
uterin în cursul sarcinii” (1939) etc. El și-a publicat
oraș.
rezultatele cercetărilor sale în reviste din Cluj, București,
Dorind să aibă un rol formativ mai important
Viena, Leipzig, Paris, Buenos Aires etc.
pentru studen i și tinerii medici, în 1938 el a devenit
El a fost membru fondator al Societă ii de
conferen iar la Clinica Ginecologică a Facultă ii de
Ginecologie, Obstetrică și Endocrinologie, întemeiată
Medicină din Cluj. Este straniu faptul că același director
în
1935 la Cluj și condusă de Cristea Grigoriu. C.
- Prof. Grigoriu - care îl eliminase pe C. Stanca din
Stanca a fost membru corespondent al Societă ii franceze
colectivul medical al Clinicii cu
18 ani înainte, și-a
de Ginecologie și membru de onoare al Asocia iei
schimbat opinia și i-a permis lui Stancă să aibă o
Contra Cancerului din Buenos Aires. De asemenea, a
importantă func ie în aceeași Clinică. A fost, oare, o
fost vicepreședinte al Asocia iei Generale a Medicilor
remușcare a lui Grigoriu? Este foarte greu de știut cauza
din România [11].
reală a acestei modi cări de atitudine a sa.
De-a lungul carierei, C. Stanca a fost distins cu
În întreaga sa carieră de la Cluj, care a avut loc între
numeroase medalii, printre care „Ordinul Ferdinand” în
anii 1929 și 1940, Stanca a fondat o „puternică școală de
grad de o er, „Coroana României” în grad de o er și,
ginecologie oncologică, ce s-a distins prin radicalism,
apoi, de comandor, Crucea „Regina Maria”, 1942 și
profesionalism, elegan ă și prin rezultate foarte bune pentru
„Meritul Sanitar” clasa I.
acea perioadă”, așa cum a arătat Ilie Neam u (1910-?)
C. Stanca a rămas în memoria celor care l-au
[5]. Este util de men ionat faptul că I. Neam u a fost
cunoscut ca un medic remarcabil, care a avut o lungă
unul dintre cei mai remarcabili discipoli ai lui C. Stanca
carieră, cu multe realizări.
și în anii ’70 a condus Sec ia de Chirurgie și Ginecologie
Nepotul său - scriitorul Horia Stanca (1909-2002)
a Institutului Oncologic din Cluj.
a notat în memoriile sale intitulate
“Fragmentarium
La izbucnirea celui de-al Doilea Război Mondial, în
Clujean” că: C. Stanca avea
„mâini agile, cu degete
septembrie 1940, C. Stanca a părăsit Clujul și s-a stabilit
sub iri, [...] lucrând cu o iu eală care mă umplea de mirare
la București. Acolo a continuat să lucreze din greu. În
pentru priceperea în mânuirea instrumentelor și amplasarea
1941, o cial rămăsese conferen iar la Facultatea de
lor la locul cuvenit în trupul [pacientei]” [12].
Medicină din Cluj, care se a a în refugiu la Sibiu. Dar
activitatea sa principală a avut loc la Spitalul „Prin ul
Nicolae” din București, unde a fost încadrat medic
Referințe
primar. El a încercat să transforme acest spital într-un
institut oncologic, dar aceasta a fost imposibil în timpul
1. Bologa VL. Un înfăptuitor: Constantin Stanca (1889-
războiului, când era o nevoie imensă de spitale militare.
1969). În Restituiri, Ed. Med. Univ.
“Iuliu
În același timp a fost medic consultant pentru bolile
Ha ieganu”, Cluj-Napoca, 2009:44-45.
prenatale la Serviciul Asigurărilor Sociale din Capitală
2. Ghibu O. La a douăzecea aniversare a Universită ii
[7]. În
1948 a întemeiat Sec ia de Maternitate a
Dacia Superioară, edi ia a II-a, îngrijită, revăzută, cu
Constantin Stanca (1889-1969) - A Prestigious Gynecologist and Oncologist of the 20th Century
161
HISTORY OF MEDICINE
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
prefa ă de Prof. Dr. Doc. Crişan Mircioiu, Ed.
7.
*** Anuarul general al medicilor din România. 1941.
Napoca Star, Cluj-Napoca, 2001:54.
Cu datele recensământului din 15 martie 1941, Tipogr.
3.
Bârsu C. Reuniunea Consiliului profesoral al Facultă ii
„Universul”, Bucureşti, 1941:256.
Româneşti de Medicină din Cluj din 1 Aprilie 1920. În
8. Ministerul Sănătă ii. Direc ia Eviden ei Documentării
Mărturii ale începutului Facultă ii de Medicină din
Statistice. Anuarul medicilor 1948, Monitorul O cial
Cluj, 1919-1920, Ed. Med. Univ. „Iuliu Ha ieganu”,
şi Imprimeriile Statului. Imprimeria Centrală,
Cluj-Napoca, 2004:139.
Bucureşti, 1948:499.
4.
Bârsu C. Întrunirea Consiliului Profesoral al Facultă ii
9.
*** Constantin Stanca. În Enciclopedia medicală
Româneşti de Medicină din Cluj din 23 Aprilie 1920.
românească, de la origini până în prezent, sub red.
În Mărturii ale începutului Facultă ii de Medicină din
Ursea N., vol. 4, Ed. Univ. “Carol Davila”, Bucureşti,
Cluj, 1919-1920: 141.
2009:2780-2781.
5.
Neam u I. Profesor Dr. Constantin Stanca
(1889-
10.
*** Lista profesorilor şi conferen iarilor în anul
1969). În Enciclopedia Oncologică: Cancerul. colului
universitar
1961/1962 la Facultă ile de Medicină,
uterin. Material de documentare şi îndrumare
Stomatologie şi Specializare şi Perfec ionare. În
metodologică, sub red. Chiricu ă I. Într. Poligr. Cluj-
Învă ământul Medical şi Farmaceutic din Bucureşti. De
Napoca, 1976:227, 228
la începuturi până în prezent, sub red. Ilea T, Ghelerter
6.
Chiricu ă I, Bolba Gh. Activitatea complexă a
I, Du escu B, Bercuş CI, Într. Poligr. „Arta Gra că”,
Institutului Oncologic Cluj-Napoca, în
guri şi
Bucureşti, 1963:566.
comentarii:
1929-1979. În Enciclopedia Oncologică,
11.
*** Facultatea de Medicină. În Anuarul Universită ii
vol.
7, Cancerul sânului. Experien a românească.
„Regele Ferdinand”, Ed.
„Cartea Românească din
Semicentenarul Institutului Oncologic Cluj-Napoca.
Cluj”, Sibiu, 1943:663-664.
Material de documentare şi îndrumare metodologică,
12. Stanca H. Anii de universitate. În Fragmentarium
Într. Poligr. Cluj-Napoca Cluj-Napoca, 1981:662.
Clujean, Ed. „Dacia”, Cluj-Napoca, 1987:87.
162
Barsu
GUIDANCE FOR DRAWING UP
STANDARDE DE REDACTARE
Scop
materiale care ar putea să îi identi ce. Dacă formularele
Revista Conexiuni Medicale publică lucrări de
de accept nu prevăd acest lucru vă rugăm să rugăm
cercetare care contribuie la progresul din toate domeniile
ob ine i acordul, sau îndepărta i posibilitatea de
medicinei. Revista publică de asemenea reviste generale,
identi care. O declara ie în acest sens trebuie inclusă în
editoriale și scurte comunicări pe domenii speci ce.
sec iunea „Metode” a lucrării.
Prezentările de caz sunt acceptate dacă prezintă interes
crescut și sunt bine investigate. Scrisorile către editor, în
Aprobarea Comitetului de Etică
special cele care prezintă o opinie privind un articol
Preciza i la sec iunea „Metode” faptul că desfășura i
publicat anterior sau care prezintă noi date, sunt de
studii asupra subiec ilor umani cu aprobarea Spitalului,
asemenea binevenite. Adresa web a revistei este http://
Comitetului de Etică al Universită ii, etc. În mod
similar, con rma i dacă experimentele asupra animalelor
trimestrial, articolele sunt acceptate în limba engleză sau
corespund standardelor etice.
română, având cel pu in traducerea în limba engleză a
rezumatului și cuvintelor cheie. Lucrările pot trimise
Asumarea dreptului de copyright
pe adresa: dr. Bumbulu Călin, editor șef adjunct,
Lucrările acceptate pentru publicare au implicit
Conexiuni Medicale, P- a. Eroilor Revolu iei nr. 23,
drepturile de copyright cedate către editor. Autorii pot
cod 440055, Satu Mare, România. Tel./Fax: +40-261-
utiliza materiale din lucrările lor în alte articole proprii,
710456, e-mail: bumbulutcalin@yahoo.com.
după ob inerea acceeptului editorului.
Republicarea articolelor
Propunerea pentru publicare
Vă rugăm să con rma i că lucrarea dumneavoastră
Toate manuscrisele propuse pentru publicare în
nu a mai fost publicată în forma prezentată sau într-o
Conexiuni Medicale vor în format compatibil pentru
formă asemănătoare, sau că nu a fost acceptată pentru
efectuarea recenziei online. Revista acceptă manuscrise
publicare într-o altă revistă.
propuse în formă electronică, în format Word (text,
guri și tabele). Nu trimite i lucrări în format PDF.
Conflicte de interese
Acceptăm lucrări care nu depășesc 3.500 de cuvinte
Rugăm autorii să declare posibilele con icte de
pentru articole originale, 2.500 pentru prezentări de
interese, inclusiv cele de natură nanciară. Dacă nu
caz, 2.000 pentru prezentări de imagini clinice, 500
există con icte de interese, vă rugăm să preciza i acest
pentru scrisori către editor și 4.500 de cuvinte pentru
lucru. Sursele de nan are trebuie precizate în lucrarea
reviste generale. Autorii NU vor trimite prin poștă sub
dumneavoastră.
formă de hârtie propunerea pentru publicare, decât
dacă este vorba de scrisori sau dacă se solicită astfel din
Permiterea de a reproduce materiale
partea redac iei. Dacă nu există altă op iune decât
publicate anterior
trimiterea prin poștă, vă rugăm să expedia i și versiunea
Vă rugăm să ne trimite i o copie a acceptului de
electronică CD-ROM pe adresa redac iei: Conexiuni
reproducere (de exemplu al ilustra iilor) de la de inătorul
Medicale, P- a. Eroilor Revolu iei nr. 23, cod 440055,
dreptului de copyright.
Satu Mare, România. Utiliza i text la două rânduri și
include i următoarele sec iuni: pagina de titlu,
Formularele de accept ale pacienților
rezumatul și cuvintele cheie, textul, mul umiri,
Protec ia drepturilor pacien ilor este esen ială; vă
referin e, tabele și guri. Paginile vor
numerotate
rugăm să ne trimite i formularele de accept ale
consecutiv, începând cu pagina de titlu, numerele
pacien ilor sau subiec ilor studiului dumneavoastră,
arabe ind plasate în col ul din dreapta sus al ecărei
prin care aceștia permit publicarea fotogra ilor sau altor
pagini.
GUIDANCE FOR DRAWING UP
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
Prezentarea lucrării
Nu recomandăm utilizarea excesivă a abrevierilor. Folosi i
Pagina de titlu
metode de calcul statistic standardizate. Nominaliza i
Cuprinde titlul întreg și titlul scurt format din
medicamentele și substan ele chimice utilizând numele
maxim 45 de caractere, numele și prenumele ecărui
generic
(dacă sunt men ionate mărcile înregistrate, se
autor; dacă lucrarea apar ine unui departament sau unei
furnizează numele producătorului și orașul).
institu ii, va men ionat numele acestuia în întregime.
Mul umiri
De asemenea numele, e-mail-ul și adresa autorului
Vor
adresate celor care au adus contribu ii
împuternicit pentru coresponden ă, sursele de nan are
importante la studiu.
sau suport utilizate sub forma burselor, echipamentelor,
Referin e
medicamentelor, sau orice combina ie a acestora.
Vor
numerotate între paranteze drepte cu
Rezumatul
numerale arabe, succesiv în ordinea în care sunt
Pagina a doua va cuprinde rezumatul cu minim 200
men ionate în text. Referin ele vor include numele
de cuvinte; nu utiliza i abrevieri, note de subsol, sau
autorilor până la al șaselea autor, dacă sunt mai mul i,
referin e.
enumera i primii trei și apoi adăuga i „et al”. Referin ele
Introducere în temă și scopuri
vor include titlul complet și sursa informa iei; numele
Descrie i importan a studiului și obiectivul
revistelor va abreviat conform Index Medicus (http://
(obiectivele) precise ale cercetării sau întrebarea
(întrebările) pe care le ridică studiul.
acceptă mai mult de 90-100 referin e; pentru scrisori
Metode
către redac ie se acceptă
5-6 referin e. Folosi i ca și
Include i informa ii privind următoarele aspecte ale
referin e cât mai pu ine rezumate. Comunicările
studiului dacă sunt utilizate: proiectul
- descrie i
personale și lucrările nepublicate nu vor men ionate la
elementele de bază ale studiului, de exemplu studiu
referin e și vor apare în text între paranteze. Lucrările
controlat randomizat, studiu cross-sec ional, de cohortă,
nepublicate dar a ate în curs de publicare vor incluse
de urmărire, serii de cazuri, etc; procedura - speci ca i
în referin e cu men iunea „in press” între paranteze,
dacă a fost desfășurat în sistem de îngrijire primar sau
lângă numele revistei implicate.
ter iar, în ambulator sau spital, în comunitate, etc;
a) Articole:
participan i - indica i numărul subiec ilor și cum au
[1] Otvos L Jr, Shao WH, Vanniasinghe AS, Amon
fost selecta i, recruta i și desemna i pentru interven ie;
MA, Holub MC, Kovalsykz I, et al. Toward understanding
interven ia
- metoda de administrare și durata
the role of leptin and leptin receptor antagonism in
interven iei.
preclinical models of rheumatoid arthritis. Peptides
Rezultate
2011;32:1567-74.
Prezenta i principalele rezultate ale studiului,
b) Lucrări publicate numai cu numerele DOI:
inclusiv intervalurile de con den ă sau valorile p.
[2] Chaldakov GN, Beltowsky J, Ghenev PI, Fiore
Concluzii
M, Panayotov P, Rancic G, et al. Adipoparacrinology -
Enun a i doar concluziile sus inute direct de dovezi,
vascular periadventitial adipose tissue (tunica adiposa) as
precum și importan a descoperirilor. Revistele generale
an example. Cell Biol Int
2011;doi:
10.1042/
și prezentările de caz vor include un rezumat
CBI20110422.
nestructurat.
c) Căr i sau manuale:
Cuvinte cheie
[3] Gertler A, editor. Leptin and Leptin Antagonists.
Rezumatul va urmat de o listă de 3-10 cuvinte
Landes Bioscience, Austin, Texas, USA. 2009.
cheie sau fraze scurte care vor ajuta la indexare. Dacă
d) Capitole de căr i sau de manuale:
este posibil, utiliza i termeni proveni i din lista Index
[4] Jeremy L, Abe PD. Treatment Options in
Medicus cu
262 subiecte medicale/Medical Subject
Super cial (pTa/pT1/CIS) Bladder Cancer. In: Urological
Headings
262
cancers in clinical practice, Springer-Verlag, London
meshhome.html).
Limited, 2007:75-102.
Textul
Tabele
Un studiu original va divizat în sec iuni denumite
Fiecare tabel va numerotat cu numerale romane,
Introducere, Metode, Rezultate și Discu ii
(incluzând
cu un titlu scurt deasupra, la subsolul lor vor trecute
concluziile), după formula „IMRAD”. Articolele lungi
notele
explicative,
men ionându-se abrevierele
pot necesita subsec iuni (în special la Rezultate și Discu ii)
nestandardizate utilizate; nominaliza i valorile statistice
pentru clari care. Alte tipuri de articole precum prezentări
care variază precum devia ia standard și eroarea standard
de caz, reviste generale, editoriale, pot urma alt format.
a medianei. Fiecare tabel va citat în text.
164
MEDICAL CONNECTIONS • NUMBER 3 (35) • OCTOBER 2014
GUIDANCE FOR DRAWING UP
Figuri
acestor sugestii, rugându-i să răspundă la întrebări și să
Toate gra cele, fotogra ile, diagramele vor
facă necesarele corec ii. Aceste informări sunt făcute în
considerate ca guri și vor numerotate succesiv în text
cel mult trei luni de la propunerea de publicare.
cu numerale arabe. Dacă o gură a fost publicată
Manuscrisul revizuit de autori va reexpediat editorului
anterior, sursa va citată cu mul umiri, men ionându-
în cel mult o lună. La primirea de către editor a versiunii
se permisiunea de inătorului de copyright. Figurile pot
corectate, înso ită de o scrisoare de răspuns punctuală la
reduse, grupate sau șterse la dorin a editorului.
comentariile recenzorilor, se retrimite manuscrisul
Legenda gurii va plasată la subsolul ei; va explicată
acelorași recenzori, care vor face recomandarea nală
scala utilizată, respectiv metodele de colorare
pentru acceptarea sau respingerea acestuia.
microscopică.
Unită i de măsură
Abonamente
Măsurătorile lungimii, înăl imii, greută ii și
Pre ul unui abonament anual pentru 2014 este: 80
volumului vor făcute în sistem metric sau multipli
RON individual, 160 RON pentru institu ii, plăti i în
decimali. Temperaturile vor
exprimate în grade
contul Colegiului Medicilor Satu Mare RO38 BTRL
Celsius. Tensiunea va
măsurată în mmHg. Toate
0310
1202 K392
62XX, cod scal
9839430, cu
măsurătorile hematologice vor exprimate în Sistemul
men iunea
„pentru abonament Conexiuni Medicale”.
Interna ional de Unită i (SI).
Solicitarea abonării poate
trimisă prin poștă: P- a.
Abrevieri și simboluri
Eroilor Revolu iei nr.
23, cod
440055, Satu Mare,
Utiliza i doar abrevieri standard. Evita i abrevierile
România. Tel./Fax: 0261-710456, 0361-408164, sau
în titlu și rezumat. Cuvântul va preceda abrevierea la
prin e-mail: colmedsm@gmail.com.
prima utilizare în text, cu excep ia unită ilor de măsură
standard.
Publicitate
Cererile pentru spa iu publicitar vor
adresate
Retipăriri
redac iei Conexiuni Medicale. Pre urile (plătite în lei la
Sunt oferite gratuit zece copii ale articolului publicat
cursul BNR) pentru publicitate pe 2014 sunt 200 euro
și două ale revistei. Dacă sunt necesare mai multe copii,
pagina (A4) color, un număr și 800 euro patru numere;
sunt disponibile contra cost.
coperta interioară fa ă sau spate: 350 euro un număr,
1400 euro patru numere; coperta exterioară spate: 400
Politica editorială
euro un număr, 1600 euro patru numere. Cont bancar:
Apreciem toate contribu iile în domeniul medicinei.
Colegiul Medicilor Satu Mare, CUI 9839430, Banca
Invităm personalită i recunoscute cu expertiză și articole
Transilvania, agen ia Golescu Satu Mare, IBAN: RO38
din diverse domenii să publice reviste generale și
BTRL 0310 1202 K392 62XX.
editoriale în revista noastră. Acceptăm de asemenea
lucrări originale și prezentări de caz din toate ările.
© Copyright Conexiuni Medicale/Medical
Conexiuni Medicale vă oferă o recenzie atentă și publicarea
Connections, Satu Mare, 2014
imediată după acceptare. Redactorii vor citi primii
Nicio parte a acestei publica ii nu poate reprodusă,
lucrarea, decizând în decurs de 1-3 săptămâni în func ie
stocată sau transmisă sub orice formă sau prin orice
de nivelul de prioritate: unele sunt trimise imediat
mijloace, fără permisiunea prealabilă în scris a revistei
recenzorilor, unele pot
respinse, iar unele sunt
Conexiuni Medicale. Permisiunea nu este necesară
returnate autorilor cu sugestii de îmbunătă ire înainte
pentru a copia rezumate sau articole dacă este indicată
de expedierea spre recenzori.
sursa, cu citarea completă a referin ei. Solicitarea
privind permisiunea de a retipări toată revista sau o
Procedura peer-review
parte a ei, va
adresată editorului prin e-mail:
Conexiuni Medicale practică o evaluare a tuturor
colmedsm@gmail.com
lucrărilor originale de către doi sau trei recenzori
independen i, din care doi sunt personalită i
Revista Conexiuni Medicale apare trimestrial prin
interna ionale. Procesul peer-review este esen ial pentru
efortul logistic și nanciar al Colegiului Medicilor
asigurarea calită ii informa iei știin i ce. Recenzorii
Satu Mare și Asocia iei Medicilor de Familie Satu
sunt ruga i să evalueze manuscrisul aplicând aceleași
Mare, în cadrul proiectului comun al Centrului de
standarde ca și pentru reviste interna ionale; comentariile
Documentare și Educa ie Medicală Continuă Satu
sunt trimise editorului, care va informa autorii asupra
Mare.
165